
Médiathèque SET

When we think of the postpartum period, pelvic floor recovery, muscle rehabilitation, and breastfeeding often come to mind. Yet, for many women, pain remains one of the greatest barriers to recovery. Pain may result from perineal trauma following vaginal birth, cesarean delivery, low back pain, neck and shoulder tension associated with breastfeeding, uterine cramping, or breastfeeding-related difficulties. These conditions can limit mobility, disrupt sleep, interfere with breastfeeding, and delay a return to daily activities. For healthcare professionals, this raises an important question: how can pain be managed effectively while ensuring treatment is safe, compatible with breastfeeding, and minimizes medication use whenever possible? EVA offers a promising solution. By combining transcutaneous electrical nerve stimulation (TENS) and neuromuscular electrical stimulation (NMES), it can address several conditions commonly encountered during the postpartum period. It may be used for both pain management and pelvic floor rehabilitation. However, the evidence supporting these applications varies. The following sections summarize what current research allows us to conclude. 1.Why TENS? TENS has been used for decades to treat musculoskeletal and postoperative pain. Its analgesic effects rely on two complementary mechanisms. At high frequencies, TENS stimulates large-diameter sensory (Aβ) fibers, reducing the transmission of nociceptive signals within the spinal cord through the gate control mechanism. At low frequencies, TENS activates descending inhibitory pathways and promotes the release of endogenous opioids. Together, these mechanisms contribute to longer-lasting analgesia (Smith et al., 2023). Recent evidence also suggests that TENS may influence inflammatory and immune responses. This mechanism may partly explain its benefits across a variety of pain conditions, including postpartum pain (Chen et al., 2025). 2.Perineal pain: the strongest evidence Perineal pain is currently the postpartum indication best supported by evidence for the use of TENS. A meta-analysis including 17 randomized controlled trials and nearly 2,000 participants found that TENS, when added to standard postpartum care, significantly reduced pain compared with standard care alone (Beleza et al., 2026). The certainty of the evidence was rated as moderate. This representing the strongest scientific support currently available for TENS in postpartum care. When TENS was compared with placebo, the findings also remained encouraging. However, the certainty of evidence was rated as very low because of methodological limitations. Clinical implications TENS can be incorporated into routine postpartum care alongside cryotherapy, positioning advice, therapeutic exercise, and analgesic medication when indicated. EVA therefore provides healthcare professionals with an additional non-pharmacological option for improving patient comfort without interfering with breastfeeding. 3.Post-cesarean pain: an adjunct to multimodal analgesia Pain after cesarean delivery can delay mobilization. It may also complicate newborn care and make breastfeeding more difficult. A Cochrane review of ten studies concluded that TENS reduces postoperative pain when used in addition to standard analgesia. Some studies also reported reduced use of rescue analgesics and improvements in physiological measures such as heart rate and respiratory rate (Zimpel et al., 2020). Clinical implications TENS is not intended to replace pharmacological analgesia. Rather, it can complement a multimodal pain management strategy aimed at improving pain control and promoting early mobilization. 4.Musculoskeletal pain: supporting functional recovery Low back, thoracic, and neck pain are common after childbirth. These symptoms are associated with pregnancy-related postural changes, infant care, breastfeeding, and the gradual return to daily activities. A review published in Frontiers in Neurology concluded that TENS effectively reduces several types of postpartum musculoskeletal pain while maintaining an excellent safety profile (Chen et al., 2025). Similarly, a network meta-analysis of pregnancy-related low back pain found significant improvements in physical function, with moderate-certainty evidence (Chen et al., 2021). Clinical implications EVA can complement therapeutic exercise, manual therapy, and postural education. Together, these interventions may promote a more comfortable recovery and facilitate a return to daily activities. 5.Pelvic floor rehabilitation: an additional advantage of EVA Pain is only one aspect of postpartum recovery. Many women also experience pelvic floor muscle weakness or difficulty activating these muscles effectively after childbirth. The NMES mode expands EVA's clinical applications. When neuromuscular electrical stimulation is indicated, it can support pelvic floor rehabilitation. For some patients, NMES may improve muscle awareness and facilitate muscle activation. It should be used alongside a supervised exercise program rather than as a stand-alone intervention. As with any rehabilitation strategy, NMES should be integrated into a comprehensive approach that includes clinical assessment, therapeutic exercise, and patient education. 6.Breast health: a promising area for future research Breastfeeding difficulties are another important source of postpartum pain. Plugged milk ducts, breast engorgement, and mastitis may interfere with breastfeeding and reduce quality of life. TENS is not currently recommended for these conditions. However, its potential is beginning to attract research interest. A case report by Smigelski and Gallagher described the use of TENS in a woman who experienced two episodes of plugged milk ducts. The authors reported rapid pain relief and complete resolution of the palpable breast mass after one or two treatment sessions. They hypothesized that electrical stimulation promoted contraction of the myoepithelial cells surrounding the mammary alveoli. This mechanism could facilitate milk ejection and help resolve ductal obstruction. How should these findings be interpreted? These findings are encouraging but should be interpreted cautiously. The report describes a single patient and did not include a control group. It also did not compare outcomes with the natural progression of the condition. Furthermore, outcomes relied primarily on patient-reported pain and clinical examination of the palpable mass. Consequently, no conclusions can be drawn regarding the effectiveness of TENS, and these findings cannot be generalized to breastfeeding women as a whole. The authors also emphasized that controlled clinical trials are needed before this approach can be recommended in clinical practice. 7.Key takeaways The postpartum period presents diverse and evolving clinical needs. Having a device that can address multiple aspects of recovery is therefore valuable for healthcare professionals. By combining TENS and NMES, EVA supports both pain management and pelvic floor rehabilitation. Current evidence particularly supports its use for: 1. Perineal pain following vaginal birth. 2. Post-cesarean pain. 3. Postpartum musculoskeletal pain. Other applications, particularly in breast health, remain investigational. Although preliminary findings are promising, high-quality clinical trials are needed before these indications can be incorporated into clinical practice guidelines. Overall, EVA is not a single solution for every postpartum challenge. Rather, it is a versatile device supported by evidence for several important indications. It can be integrated into a comprehensive, individualized, and woman-centred approach to postpartum care. Références: Beleza, A. C. S., Jorge, C. H., Liebano, R. E., et al. (2026). Electrophysical resources for the treatment of acute perineal pain after vaginal delivery: A systematic review with meta-analysis. The Journal of Pain. Bernard, A., Oyler, D. R., Anglen, J. O., et al. (2020). Best practices guidelines for acute pain management in trauma patients. American College of Surgeons. Chen, B., Chen, C., Zhao, X., & Xu, Y. (2025). An update comprehensive review on the effects of transcutaneous electrical nerve stimulation for postnatal physical and psychological disorders. Frontiers in Neurology. Chen, L., Ferreira, M. L., Beckenkamp, P. R., et al. (2021). Comparative efficacy and safety of conservative care for pregnancy-related low back pain: A systematic review and network meta-analysis. Physical Therapy. Deussen, A. R., Ashwood, P., Martis, R., Stewart, F., & Grzeskowiak, L. E. (2020). Relief of pain due to uterine cramping/involution after birth. Cochrane Database of Systematic Reviews. Gibson, W., Wand, B. M., Meads, C., Catley, M. J., & O'Connell, N. E. (2019). Transcutaneous electrical nerve stimulation (TENS) for chronic pain: An overview of Cochrane reviews. Cochrane Database of Systematic Reviews. Martimbianco, A. L. C., Porfírio, G. J., Pacheco, R. L., Torloni, M. R., & Riera, R. (2019). Transcutaneous electrical nerve stimulation (TENS) for chronic neck pain. Cochrane Database of Systematic Reviews. McCahill-Riley, M., Downey, K., & Clarke, V. (2026). Electrotherapy in lactation care. Journal of Human Lactation. Smith, T. J., Wang, E. J., & Loprinzi, C. L. (2023). Cutaneous electroanalgesia for relief of chronic and neuropathic pain. The New England Journal of Medicine. Smigelski, C., & Gallagher, L. (2024). The use of transcutaneous electrical nerve stimulation (TENS) to relieve pain and resolve blocked milk ducts in lactating women: A case report [Affiche scientifique]. Oregon Health & Science University. Zimpel, S. A., Torloni, M. R., Porfírio, G. J., Flumignan, R. L., & da Silva, E. M. (2020). Complementary and alternative therapies for post-caesarean pain. Cochrane Database of Systematic Reviews.
Lorsqu'on pense au postpartum, on pense spontanément au plancher pelvien, à la récupération musculaire ou à l'allaitement. Pourtant, pour plusieurs femmes, l’un des principaux obstacles à la récupération demeure la douleur : douleur périnéale après un accouchement vaginal, douleur post-césarienne, lombalgies, tensions cervicales liées à l'allaitement, crampes utérines ou inconfort associé aux difficultés d'allaitement... Ces douleurs peuvent limiter la mobilité, nuire au sommeil, compliquer l'allaitement et retarder le retour aux activités. Pour les professionnels de la santé, cela soulève une question importante : comment offrir des traitements efficaces, sécuritaires, compatibles avec l'allaitement et permettant de limiter le recours à la médication lorsque cela est possible ? C'est dans cette perspective que le EVA présente un intérêt. En combinant la stimulation électrique transcutanée (TENS) et la stimulation électrique neuromusculaire (NMES), il permet d'accompagner plusieurs problématiques fréquemment rencontrées en postpartum, qu'il s'agisse de la gestion de la douleur ou de rééducation du plancher pelvien. Toutes les indications ne reposent toutefois pas sur le même niveau de preuve. Voici ce que la littérature scientifique permet actuellement de conclure. 1.Pourquoi le TENS? Le TENS est utilisé depuis plusieurs décennies pour traiter les douleurs musculosquelettiques et postopératoire. Son efficacité repose principalement sur deux mécanismes complémentaires. À haute fréquence, il stimule les fibres sensitives de gros diamètre (Aβ), ce qui réduit la transmission des signaux douloureux au niveau de la moelle épinière selon le mécanisme du portillon spinal. À basse fréquence, il active également les voies inhibitrices descendantes et favorise la libération d'opioïdes endogènes, contribuant ainsi à une analgésie plus prolongée (Smith et al., 2023). Une revue récente suggère également que le TENS pourrait moduler certaines réponses inflammatoires et immunitaires, ce qui pourrait expliquer une partie des effets bénéfiques observés dans différents contextes douloureux, notamment en postpartum (Chen et al., 2025). 2.Douleur périnéale : l'indication la mieux soutenue La douleur périnéale constitue actuellement l'indication du TENS la mieux étayée par les données probantes chez les femmes en postpartum. Une méta-analyse regroupant 17 essais cliniques et près de 2 000 participantes rapporte que le TENS, utilisé en complément des soins habituels, réduit significativement la douleur comparativement aux soins habituels seuls (Beleza et al., 2026). Les auteurs jugent le niveau de preuve modéré, ce qui en fait l'indication postpartum bénéficiant actuellement du soutien scientifique le plus solide. Lorsque le TENS est comparé à un placebo, les résultats demeurent encourageants, mais le niveau de preuve est considéré comme très faible en raison de plusieurs limites méthodologiques. Ce que cela signifie en clinique Le TENS peut être intégré aux traitements habituels, notamment la cryothérapie, les conseils de positionnement, les exercices thérapeutiques et la médication, lorsque nécessaire. Pour les professionnels de la santé, le EVA représente ainsi une option supplémentaire pour améliorer le confort des patientes, sans interférer avec l'allaitement. 3.Douleur post-césarienne : un complément à l'analgésie multimodale La douleur après une césarienne peut retarder la mobilisation, compliquer les soins au nouveau-né et rendre l'allaitement plus difficile. Une revue Cochrane regroupant dix études conclut que le TENS réduit la douleur postopératoire lorsqu'il est utilisé en complément de l'analgésie habituelle. Certaines études rapportent également une diminution des recours aux analgésiques de secours ainsi qu'une amélioration de certains paramètres physiologiques, comme la fréquence cardiaque et respiratoire (Zimpel et al., 2020). Ce que cela signifie en clinique Le TENS ne remplace pas l'analgésie pharmacologique. Il peut toutefois peut s'intégrer à une approche multimodale visant à optimiser le contrôle de la douleur et à favoriser une mobilisation précoce. 4.Douleurs musculosquelettiques : accompagner la reprise des activités Les douleurs lombaires, thoraciques et cervicales sont très fréquentes après l'accouchement. Elles sont associées aux adaptations liées à la grossesse, au portage du bébé, à l'allaitement et à la reprise graduelle des activités. Une revue publiée dans Frontiers in Neurology conclut que le TENS est efficace pour soulager plusieurs douleurs musculosquelettiques rencontrées en postpartum, tout en présentant un excellent profil d'innocuité (Chen et al., 2025). Par ailleurs, une méta-analyse en réseau portant sur la lombalgie liée à la grossesse rapporte une amélioration significative de la fonction physique, avec un niveau de preuve modéré (Chen et al., 2021). Ce que cela signifie en clinique Le EVA peut être utilisé en complément des exercices thérapeutiques, de la thérapie manuelle et de l'éducation posturale afin de favoriser une récupération plus confortable et de faciliter le retour aux activités quotidiennes. 5.La rééducation du plancher pelvien : un autre atout du EVA La douleur n'est pas le seul enjeu du postpartum. Après l'accouchement, plusieurs femmes présentent également une faiblesse du plancher pelvien ou une difficulté à recruter efficacement cette musculature. Grâce à son mode NMES, EVA peut également soutenir la rééducation du plancher pelvien lorsqu'une stimulation neuromusculaire est cliniquement indiquée. Chez certaines patientes, cette modalité peut favoriser une meilleure prise de conscience musculaire et faciliter l'exécution d'un programme d'exercices supervisés. Comme toute intervention en réadaptation, la NMES doit s'inscrire dans une approche globale comprenant l'évaluation clinique, les exercices thérapeutiques et l'éducation de la patiente. 6.Santé mammaire : une avenue de recherche prometteuse Les difficultés liées à l'allaitement constituent une autre source importante de douleur en postpartum. Les canaux lactifères obstrués, l'engorgement mammaire et la mastite peuvent compromettre la poursuite de l'allaitement et nuire à la qualité de vie. Bien que le TENS ne fasse pas partie des traitements actuellement recommandés pour ces conditions, certaines équipes de recherche commencent à en explorer le potentiel. Une étude de cas présentée par Smigelski et Gallagher décrit l'utilisation du TENS chez une femme ayant présenté deux épisodes de canaux lactifères obstrués. Les auteurs rapportent une diminution rapide de la douleur ainsi que la disparition complète de la masse palpable après une ou deux séances de traitement. Ils avancent l'hypothèse que la stimulation favoriserait la contraction des cellules myoépithéliales entourant les alvéoles mammaires, facilitant ainsi l'éjection du lait et la résolution de l'obstruction. Comment interpréter ces résultats? Bien que ces résultats soient encourageants, ils doivent être interprétés avec prudence. Cette publication décrit le cas d'une seule patiente, sans groupe témoin ni comparaison avec l'évolution naturelle de la condition. De plus, les résultats reposent principalement sur la douleur rapportée par la patiente et sur l'évaluation clinique de la masse palpable. Il est donc impossible de conclure à l'efficacité du TENS ou de généraliser ces observations à l'ensemble des femmes allaitantes. Les auteurs soulignent d'ailleurs que des essais cliniques contrôlés sont nécessaires avant qu'une telle approche puisse être recommandée en pratique clinique. 7.Ce qu'il faut retenir Le postpartum est une période caractérisée par des besoins cliniques multiples et évolutifs. Pour les professionnels de la santé, disposer d'un appareil capable d'accompagner différentes étapes de cette récupération représente un avantage. Grâce à ses modes TENS et NMES, EVA permet d'intervenir à la fois dans la prise en charge de la douleur et dans la rééducation du plancher pelvien. Les données probantes soutiennent particulièrement son utilisation pour : 1. la douleur périnéale après un accouchement vaginal; 2. la douleur post-césarienne; 3. les douleurs musculosquelettiques liées au postpartum. D'autres applications, notamment en santé mammaire, suscitent un intérêt croissant, mais reposent encore sur des données préliminaires. Elles devront être confirmées par des essais cliniques de qualité avant de pouvoir être intégrées aux recommandations de pratique. En somme, le EVA ne constitue pas une solution unique à toutes les problématiques du postpartum. Il représente plutôt un outil polyvalent dont plusieurs indications sont appuyées par les données probantes et qui peut s'intégrer à une prise en charge globale, personnalisée et centrée sur les besoins des femmes. Références: Beleza, A. C. S., Jorge, C. H., Liebano, R. E., et al. (2026). Electrophysical resources for the treatment of acute perineal pain after vaginal delivery: A systematic review with meta-analysis. The Journal of Pain. Bernard, A., Oyler, D. R., Anglen, J. O., et al. (2020). Best practices guidelines for acute pain management in trauma patients. American College of Surgeons. Chen, B., Chen, C., Zhao, X., & Xu, Y. (2025). An update comprehensive review on the effects of transcutaneous electrical nerve stimulation for postnatal physical and psychological disorders. Frontiers in Neurology. Chen, L., Ferreira, M. L., Beckenkamp, P. R., et al. (2021). Comparative efficacy and safety of conservative care for pregnancy-related low back pain: A systematic review and network meta-analysis. Physical Therapy. Deussen, A. R., Ashwood, P., Martis, R., Stewart, F., & Grzeskowiak, L. E. (2020). Relief of pain due to uterine cramping/involution after birth. Cochrane Database of Systematic Reviews. Gibson, W., Wand, B. M., Meads, C., Catley, M. J., & O'Connell, N. E. (2019). Transcutaneous electrical nerve stimulation (TENS) for chronic pain: An overview of Cochrane reviews. Cochrane Database of Systematic Reviews. Martimbianco, A. L. C., Porfírio, G. J., Pacheco, R. L., Torloni, M. R., & Riera, R. (2019). Transcutaneous electrical nerve stimulation (TENS) for chronic neck pain. Cochrane Database of Systematic Reviews. McCahill-Riley, M., Downey, K., & Clarke, V. (2026). Electrotherapy in lactation care. Journal of Human Lactation. Smith, T. J., Wang, E. J., & Loprinzi, C. L. (2023). Cutaneous electroanalgesia for relief of chronic and neuropathic pain. The New England Journal of Medicine. Smigelski, C., & Gallagher, L. (2024). The use of transcutaneous electrical nerve stimulation (TENS) to relieve pain and resolve blocked milk ducts in lactating women: A case report [Affiche scientifique]. Oregon Health & Science University. Zimpel, S. A., Torloni, M. R., Porfírio, G. J., Flumignan, R. L., & da Silva, E. M. (2020). Complementary and alternative therapies for post-caesarean pain. Cochrane Database of Systematic Reviews.

La NMES en phase préopératoire de l'épaule
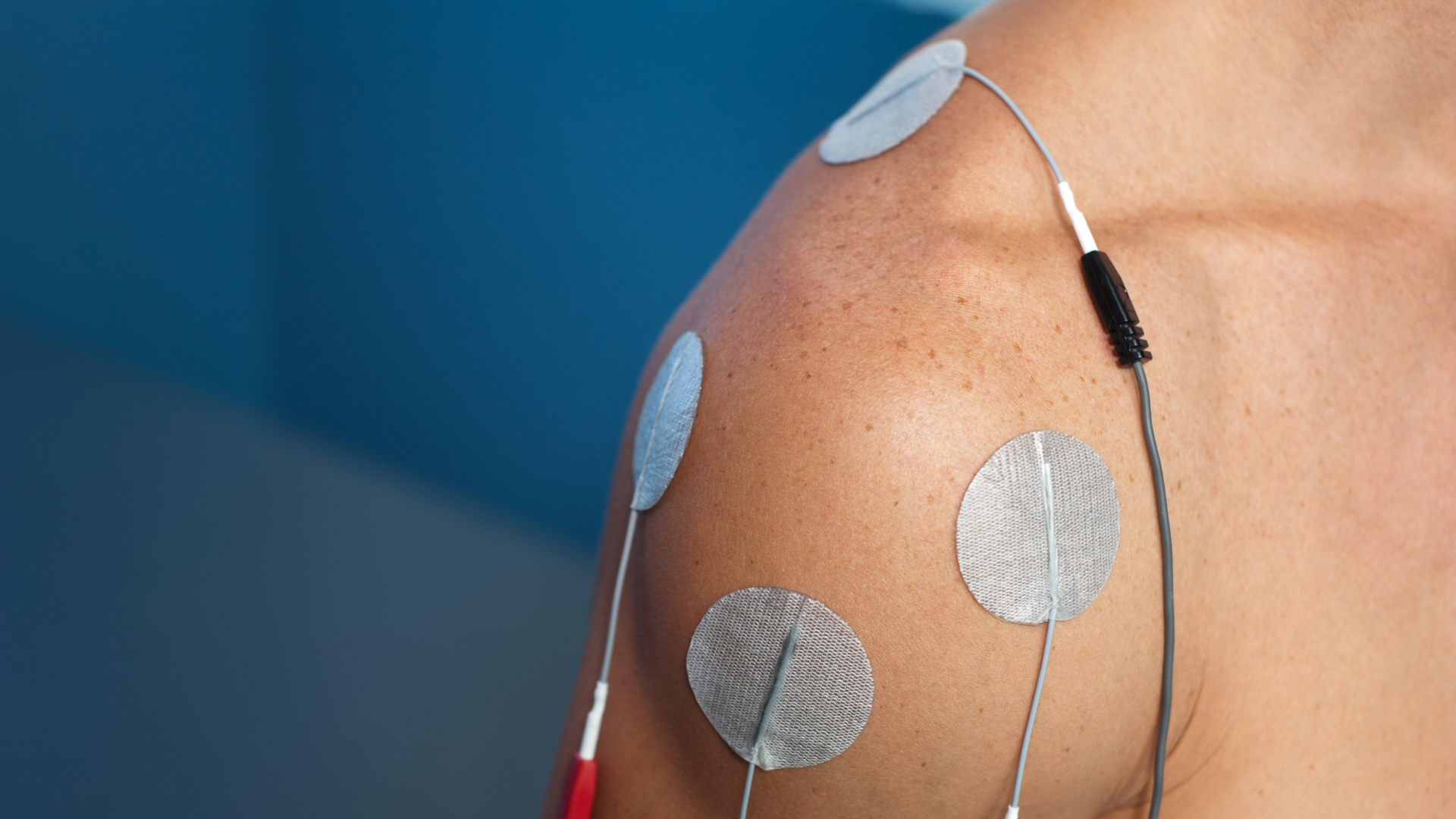
Neuromuscular electrical stimulation (NMES) is often associated with postoperative rehabilitation. However, growing evidence suggests that introducing NMES before surgery can play a meaningful role in improving patient outcomes (Punnoose et al., 2023; Walls et al., 2010; Patanè et al., 2025). This approach is based on a simple principle: the patient’s muscular status at the time of surgery influences postoperative recovery (Gillis et al., 2022; Hiyama et al., 2026). In other words, better preoperative muscle function is generally associated with better functional outcomes after surgery (Punnoose et al., 2023; Devasenapathy et al., 2019). This concept, often summarized as Better In, Better Out, is now supported by robust evidence across several orthopedic settings (Gillis et al., 2022; Jørgensen et al., 2024). Preoperative Muscle Strength: A Modifiable Prognostic Factor Among the many factors that influence recovery after orthopedic surgery, preoperative muscle strength stands out for two reasons. It is strongly associated with postoperative outcomes (Devasenapathy et al., 2019; Takamura et al., 2024; Hiyama et al., 2026), and it can be improved before surgery (Punnoose et al., 2023; Walls et al., 2010). Total Knee Arthroplasty In patients undergoing total knee arthroplasty, preoperative quadriceps strength is one of the strongest predictors of postoperative function (Devasenapathy et al., 2019; Hiyama et al., 2026). Patients with greater strength before surgery are more likely to achieve satisfactory mobility and functional recovery. Several studies have identified strength thresholds that predict walking ability six months after surgery (Takamura et al., 2024). More recently, Hiyama and colleagues (2026) reported that patients who regain age-adjusted normative quadriceps strength experience greater satisfaction and better functional outcomes one year after surgery. Anterior Cruciate Ligament Reconstruction A similar pattern is seen after anterior cruciate ligament reconstruction. Significant preoperative quadriceps weakness is associated with poorer knee function one year after surgery (Kim et al., 2022). Conversely, patients with greater preoperative strength tend to achieve better functional outcomes. These findings are consistent with the conclusions of a recent systematic review (Qiu et al., 2020). Shoulder Surgery Preoperative muscle strength also plays an important role in shoulder surgery. In patients undergoing anatomic or reverse shoulder arthroplasty, abduction and external rotation strength are among the strongest predictors of postoperative function (Hao et al., 2022a; Hao et al., 2022b). Grip strength, often considered a global indicator of muscle health and sarcopenia, has also been associated with outcomes following shoulder arthroplasty (Lee et al., 2023). More recent evidence suggests that it may also predict functional recovery after rotator cuff repair. NMES: An Opportunity Before Surgery If muscle strength affects postoperative outcomes, an obvious question arises: can this factor be optimized before surgery? NMES represents an attractive option, particularly for patients with pain, marked weakness, or functional limitations that restrict conventional exercise. In a pilot study involving patients awaiting total knee arthroplasty, a home-based NMES program increased quadriceps strength by approximately 28% before surgery (Walls et al., 2010). These gains translated into faster recovery of strength and function in the early postoperative period, while also limiting muscle atrophy. These findings align with the broader evidence supporting prehabilitation. A meta-analysis published in JAMA Network Open, which included 48 randomized controlled trials and more than 3,500 participants, found that preoperative interventions significantly improved muscle strength and physical function before surgery. Benefits persisted during the first weeks of postoperative recovery (Punnoose et al., 2023). The Role of NMES After Surgery NMES remains a valuable tool after surgery. During the early postoperative period, muscle recovery is limited by pain, joint effusion, immobilization, arthrogenic muscle inhibition, and reduced physical activity. In this context, NMES can effectively stimulate muscle activation despite these limitations. Following Knee Surgery After arthroplasty or ligament reconstruction, rapid quadriceps weakness represents a major clinical challenge. Early use of NMES may help attenuate strength loss and accelerate functional recovery, particularly when voluntary activation remains impaired. Following Shoulder Surgery Although evidence of preoperative NMES in shoulder surgery remains limited, postoperative findings are encouraging. Recent studies have shown that NMES may reduce deltoid atrophy after rotator cuff repair and accelerate recovery of abduction strength (Yoon et al., 2026). Other studies have reported earlier improvements in external rotation strength when NMES is applied to the infraspinatus during the initial phases of rehabilitation (Reinold et al., 2008). Sarcopenia: An Often Overlooked Factor Beyond muscle strength, preoperative muscle mass also appears to influence outcomes. A meta-analysis including more than 14,000 patients found that low preoperative muscle mass was associated with a significantly higher risk of major postoperative complications and short-term mortality (Weerink et al., 2020). In total knee arthroplasty, low muscle mass has also been identified as an independent risk factor for postoperative blood transfusion (Hwang et al., 2022). These findings highlight that preoperative preparation is not solely aimed at improving function. It may also help reduce surgical risk. Key Takeaways Current evidence points to a consistent conclusion: preoperative muscle status has a direct impact on recovery following orthopedic surgery. For rehabilitation professionals, this represents an opportunity to intervene before the operation takes place. NMES appears particularly valuable for optimizing a modifiable prognostic factor, especially when pain or functional limitations prevent patients from performing high-intensity strengthening exercises. From this perspective, the period leading up to surgery should no longer be viewed as passively waiting. Instead, it should be considered a therapeutic window during which clinicians can improve a patient’s muscle reserve, support postoperative recovery, and ultimately enhance functional outcomes. In orthopedic rehabilitation, recovery often begins long before the patient enters the operating room. References Bodkin, S. G., Norte, G. E., & Hart, J. M. (2019). Corticospinal excitability can discriminate quadriceps strength indicative of knee function after ACL-reconstruction. Scandinavian Journal of Medicine & Science in Sports, 29(5), 716–724. Devasenapathy, N., Maddison, R., Malhotra, R., Zodepy, S., & Sharma, S. (2019). Preoperative quadriceps muscle strength and functional ability predict performance-based outcomes 6 months after total knee arthroplasty: A systematic review. Physical Therapy, 99(1), 46–61. Gillis, C., Ljungqvist, O., & Carli, F. (2022). Prehabilitation, enhanced recovery after surgery, or both? A narrative review. British Journal of Anaesthesia, 128(3), 434–448. Hao, K. A., Wright, T. W., Schoch, B. S., Struk, A. M., King, J. J., & Farmer, K. W. (2022a). Association between preoperative shoulder strength and clinical outcomes after primary reverse total shoulder arthroplasty. Journal of the American Academy of Orthopaedic Surgeons, 30(15), e1035–e1044. Hao, K. A., Wright, T. W., Dean, E. W., Struk, A. M., & King, J. J. (2022b). Preoperative shoulder strength is associated with postoperative primary anatomic total shoulder arthroplasty outcomes and improvement. Journal of Shoulder and Elbow Surgery, 31(8), 1648–1656. Hauger, A. V., Reiman, M. P., Bjordal, J. M., Sheets, C., Ledbetter, L., & Goode, A. P. (2018). Neuromuscular electrical stimulation is effective in strengthening the quadriceps muscle after anterior cruciate ligament surgery. Knee Surgery, Sports Traumatology, Arthroscopy, 26(2), 399–410. Hiyama, Y., Sawa, R., Yokoyama, M., & Ishii, Y. (2026). Achieving normative quadriceps strength after total knee arthroplasty: Associations with satisfaction, function, and a predictive nomogram. The Bone & Joint Journal, 108-B(1), 45–52. Hwang, D., Han, H. S., Lee, M. C., & Ro, D. H. (2022). Low muscle mass is an independent risk factor for postoperative blood transfusion in total knee arthroplasty: A retrospective, propensity score-matched cohort study. BMC Geriatrics, 22(1), Article 137. Jenssen, K. K., Lundgreen, K., Madsen, J. E., Kvakestad, R., & Dimmen, S. (2018). Prognostic factors for functional outcome after rotator cuff repair: A prospective cohort study with 2-year follow-up. The American Journal of Sports Medicine, 46(14), 3504–3510. Jørgensen, S. L., Aagaard, P., Bohn, M. B., Mikkelsen, L. R., & Mechlenburg, I. (2024). The effect of blood flow restriction exercise prior to total knee arthroplasty on postoperative physical function, lower limb strength and patient-reported outcomes: A randomized controlled trial. Scandinavian Journal of Medicine & Science in Sports, 34(1), e14516. Kim, D. K., Park, G., Wang, J. H., Kuo, L. T., & Park, W. H. (2022). Preoperative quadriceps muscle strength deficit severity predicts knee function one year after anterior cruciate ligament reconstruction. Scientific Reports, 12(1), Article 11845. Lee, B. G., Lee, D., & Koh, J. H. (2023). Relationship between the preoperative grip strength and postoperative shoulder strength of patients treated via reverse shoulder arthroplasty. Journal of Shoulder and Elbow Surgery, 32(5), 1012–1019. Patanè, P., Carnevale Pellino, V., Febbi, M., Gatti, R., & Sirtori, V. (2025). Effects of a tele-prehabilitation program with indirect electrostimulation compared to home-based exercise in patients eligible for lower limb arthroplasty: A randomized controlled trial. Journal of Clinical Medicine, 14(3), Article 892. Punnoose, A., Claydon-Mueller, L. S., Weiss, O., Zhang, J., Maffulli, N., & Rushton, A. (2023). Takamura, D., Iwata, K., Yajima, Y., et al. (2024). Cut-off values of preoperative knee extensor strength and hip abductor strength for predicting good walking ability after total knee arthroplasty. Archives of Orthopaedic and Trauma Surgery, 144(1), 305–312. Walls, R. J., McHugh, G., O'Gorman, D. J., Moyna, N. M., & O'Byrne, J. M. (2010). Effects of preoperative neuromuscular electrical stimulation on quadriceps strength and functional recovery in total knee arthroplasty: A pilot study. BMC Musculoskeletal Disorders, 11, 119.
On associe souvent la stimulation électrique neuromusculaire (NMES) à la phase postopératoire. Cependant, des preuves de plus en plus convaincantes indiquent que son utilisation précoce, avant l’intervention chirurgicale, peut contribuer significativement à la réadaptation des patients (Punnoose et al., 2023 ; Walls et al., 2010 ; Patanè et al., 2025). Cette évolution repose sur une idée simple : l'état musculaire dans lequel un patient entre en chirurgie influence directement sa capacité à récupérer par la suite (Gillis et al., 2022 ; Hiyama et al., 2026). En d'autres termes, une meilleure condition musculaire préopératoire est généralement associée à de meilleurs résultats fonctionnels postopératoires (Punnoose et al., 2023 ; Devasenapathy et al., 2019). Ce principe, parfois résumé par l'expression Better In, Better Out, est aujourd'hui soutenu par des données robustes dans plusieurs contextes orthopédiques (Gillis et al., 2022 ; Jørgensen et al., 2024). La force musculaire préopératoire : un facteur pronostique modifiable Parmi les nombreux facteurs susceptibles d'influencer la récupération après une chirurgie orthopédique, la force musculaire préopératoire se distingue par deux caractéristiques importantes : elle est fortement associée aux résultats postopératoires (Devasenapathy et al., 2019 ; Takamura et al., 2024 ; Hiyama et al., 2026) et elle peut être améliorée avant l'intervention. (Punnoose et al., 2023 ; Walls et al., 2010) Arthroplastie totale du genou Chez les personnes qui subissent une arthroplastie totale du genou, la force du quadriceps avant l'opération est l'un des meilleurs prédicteurs de la récupération fonctionnelle ultérieure (Devasenapathy et al., 2019; Hiyama et al., 2026). Les patients présentant une meilleure force musculaire avant la chirurgie ont davantage de chances d'atteindre des niveaux satisfaisants de fonction et de mobilité après l'intervention. Certaines études ont même identifié des seuils de force permettant de prédire la capacité de marche à six mois postopératoires (Takamura et al., 2024). Plus récemment, Hiyama et ses collègues (2026) ont montré que les patients qui retrouvent une force du quadriceps comparable aux valeurs normatives rapportent une meilleure satisfaction et de meilleurs résultats fonctionnels un an après leur chirurgie. Reconstruction du ligament croisé antérieur La même tendance est observée après une reconstruction du ligament croisé antérieur. Un déficit préopératoire important de force du quadriceps est associé à une moins bonne fonction du genou à un an (Kim et al., 2022). À l'inverse, les patients qui présentent une meilleure force musculaire avant l'intervention obtiennent généralement de meilleurs résultats fonctionnels postopératoires. Cette association est également appuyée par les conclusions d'une revue systématique récente (Qiu et al., 2020). Chirurgies de l'épaule À l'épaule, la force musculaire préopératoire joue également un rôle déterminant. Chez les patients qui subissent une arthroplastie anatomique ou inversée, la force en abduction et en rotation externe figure parmi les prédicteurs les plus puissants des résultats fonctionnels postopératoires (Hao et al., 2022a; Hao et al., 2022b). La force de préhension, souvent considérée comme un indicateur global de l'état musculaire et de la sarcopénie, s'avère également associée aux résultats postopératoires après arthroplastie de l'épaule (Lee et al., 2023). Plus récemment, des données suggèrent qu'elle pourrait aussi prédire la récupération fonctionnelle après réparation de la coiffe des rotateurs. La SNME : une occasion d'agir avant la chirurgie Si la force musculaire influence le pronostic postopératoire, la question devient alors évidente : peut-on améliorer ce facteur avant l'intervention? La NMES constitue une avenue particulièrement intéressante pour y parvenir, notamment chez les patients qui présentent de la douleur, une faiblesse importante ou des limitations fonctionnelles qui restreignent leur capacité à s'entraîner de façon conventionnelle. Dans une étude pilote réalisée auprès de patients en attente d'une arthroplastie totale du genou, un programme de NMES à domicile a permis d'augmenter la force du quadriceps d'environ 28 % avant la chirurgie (Walls et al., 2010). Ces gains se sont traduits par une récupération plus rapide de la force et de la fonction durant les semaines suivant l'intervention, tout en limitant l'atrophie musculaire postopératoire. Ces résultats s'inscrivent dans un ensemble de données plus large soutenant les bénéfices de la préhabilitation. Une méta-analyse publiée dans JAMA Network Open, regroupant 48 essais cliniques et plus de 3 500 participants, a démontré que les interventions réalisées avant la chirurgie améliorent significativement la force musculaire et la fonction préopératoires, avec des bénéfices qui se maintiennent durant les premières semaines de récupération postopératoire (Punnoose et al., 2023). Le rôle de la SNME après la chirurgie La NMES demeure toutefois un outil pertinent après l'intervention. Au cours des premières semaines postopératoires, plusieurs facteurs limitent la récupération musculaire : douleur, épanchement articulaire, immobilisation, inhibition musculaire réflexe et réduction de l'activité physique. Dans ce contexte, la NMES permet de solliciter efficacement le muscle malgré les limitations fonctionnelles présentes. Après une chirurgie du genou Après une arthroplastie ou une reconstruction ligamentaire, la perte rapide de force du quadriceps représente un défi clinique majeur. L'utilisation précoce de la NMES peut contribuer à atténuer cette perte et favoriser une récupération fonctionnelle plus rapide, particulièrement lorsque l'activation volontaire demeure insuffisante. Après une chirurgie de l'épaule Bien que les données sur la NMES préopératoire à l'épaule soient encore limitées, les résultats postopératoires sont prometteurs. Des études récentes démontrent que la NMES peut réduire l'atrophie du deltoïde après une réparation de la coiffe des rotateurs et accélérer la récupération de la force en abduction (Yoon et al., 2026). D'autres travaux ont également observé une amélioration précoce de la force en rotation externe lorsque la NMES est appliquée à l'infraépineux durant les premières phases de réadaptation (Reinold et al., 2008). La sarcopénie : un facteur souvent sous-estimé Au-delà de la force musculaire, la quantité de masse musculaire disponible avant la chirurgie semble également influencer les résultats. Une méta-analyse regroupant plus de 14 000 patients a montré qu'une faible masse musculaire préopératoire est associée à une augmentation significative du risque de complications postopératoires majeures et de mortalité à court terme (Weerink et al., 2020). En arthroplastie du genou, une faible masse musculaire a également été identifiée comme un facteur de risque indépendant de transfusion postopératoire (Hwang et al., 2022). Ces observations rappellent que la préparation préopératoire ne vise pas uniquement à améliorer la fonction. Elle peut également contribuer à réduire certains risques associés à l'intervention chirurgicale. Ce qu'il faut retenir Les données actuelles convergent vers un même constat : la condition musculaire préopératoire influence directement la récupération après une chirurgie orthopédique. Pour les professionnels de la réadaptation, cela représente une occasion importante d'agir avant même que l'intervention n'ait lieu. La NMES apparaît comme une stratégie particulièrement intéressante pour optimiser un facteur pronostique modifiable, surtout lorsque la douleur ou les limitations fonctionnelles compromettent la capacité du patient à réaliser un entraînement musculaire suffisamment intense. Dans cette perspective, la période précédant la chirurgie ne devrait plus être considérée comme une simple attente. Elle constitue plutôt une fenêtre thérapeutique où il est possible d'améliorer la réserve musculaire du patient, de favoriser sa récupération future et, ultimement, d'optimiser ses résultats fonctionnels. Parce qu'en réadaptation orthopédique, la récupération commence souvent bien avant l'entrée en salle d'opération. Bodkin, S. G., Norte, G. E., & Hart, J. M. (2019). Corticospinal excitability can discriminate quadriceps strength indicative of knee function after ACL-reconstruction. Scandinavian Journal of Medicine & Science in Sports, 29(5), 716–724. Devasenapathy, N., Maddison, R., Malhotra, R., Zodepy, S., & Sharma, S. (2019). Preoperative quadriceps muscle strength and functional ability predict performance-based outcomes 6 months after total knee arthroplasty: A systematic review. Physical Therapy, 99(1), 46–61. Gillis, C., Ljungqvist, O., & Carli, F. (2022). Prehabilitation, enhanced recovery after surgery, or both? A narrative review. British Journal of Anaesthesia, 128(3), 434–448. Hao, K. A., Wright, T. W., Schoch, B. S., Struk, A. M., King, J. J., & Farmer, K. W. (2022a). Association between preoperative shoulder strength and clinical outcomes after primary reverse total shoulder arthroplasty. Journal of the American Academy of Orthopaedic Surgeons, 30(15), e1035–e1044. Hao, K. A., Wright, T. W., Dean, E. W., Struk, A. M., & King, J. J. (2022b). Preoperative shoulder strength is associated with postoperative primary anatomic total shoulder arthroplasty outcomes and improvement. Journal of Shoulder and Elbow Surgery, 31(8), 1648–1656. Hauger, A. V., Reiman, M. P., Bjordal, J. M., Sheets, C., Ledbetter, L., & Goode, A. P. (2018). Neuromuscular electrical stimulation is effective in strengthening the quadriceps muscle after anterior cruciate ligament surgery. Knee Surgery, Sports Traumatology, Arthroscopy, 26(2), 399–410. Hiyama, Y., Sawa, R., Yokoyama, M., & Ishii, Y. (2026). Achieving normative quadriceps strength after total knee arthroplasty: Associations with satisfaction, function, and a predictive nomogram. The Bone & Joint Journal, 108-B(1), 45–52. Hwang, D., Han, H. S., Lee, M. C., & Ro, D. H. (2022). Low muscle mass is an independent risk factor for postoperative blood transfusion in total knee arthroplasty: A retrospective, propensity score-matched cohort study. BMC Geriatrics, 22(1), Article 137. Jenssen, K. K., Lundgreen, K., Madsen, J. E., Kvakestad, R., & Dimmen, S. (2018). Prognostic factors for functional outcome after rotator cuff repair: A prospective cohort study with 2-year follow-up. The American Journal of Sports Medicine, 46(14), 3504–3510. Jørgensen, S. L., Aagaard, P., Bohn, M. B., Mikkelsen, L. R., & Mechlenburg, I. (2024). The effect of blood flow restriction exercise prior to total knee arthroplasty on postoperative physical function, lower limb strength and patient-reported outcomes: A randomized controlled trial. Scandinavian Journal of Medicine & Science in Sports, 34(1), e14516. Kim, D. K., Park, G., Wang, J. H., Kuo, L. T., & Park, W. H. (2022). Preoperative quadriceps muscle strength deficit severity predicts knee function one year after anterior cruciate ligament reconstruction. Scientific Reports, 12(1), Article 11845. Lee, B. G., Lee, D., & Koh, J. H. (2023). Relationship between the preoperative grip strength and postoperative shoulder strength of patients treated via reverse shoulder arthroplasty. Journal of Shoulder and Elbow Surgery, 32(5), 1012–1019. Patanè, P., Carnevale Pellino, V., Febbi, M., Gatti, R., & Sirtori, V. (2025). Effects of a tele-prehabilitation program with indirect electrostimulation compared to home-based exercise in patients eligible for lower limb arthroplasty: A randomized controlled trial. Journal of Clinical Medicine, 14(3), Article 892. Punnoose, A., Claydon-Mueller, L. S., Weiss, O., Zhang, J., Maffulli, N., & Rushton, A. (2023). Takamura, D., Iwata, K., Yajima, Y., et al. (2024). Cut-off values of preoperative knee extensor strength and hip abductor strength for predicting good walking ability after total knee arthroplasty. Archives of Orthopaedic and Trauma Surgery, 144(1), 305–312. Walls, R. J., McHugh, G., O'Gorman, D. J., Moyna, N. M., & O'Byrne, J. M. (2010). Effects of preoperative neuromuscular electrical stimulation on quadriceps strength and functional recovery in total knee arthroplasty: A pilot study. BMC Musculoskeletal Disorders, 11, 119.

Pain in the back, neck, shoulder, or knee is very common. In most cases, pain improves over time. However, in some situations, it can last for several months and become chronic. The good news is that it is often possible to take action early to reduce this risk. Why Does Some Pain Become Chronic? Pain does not depend solely on an injury or a physical problem. Several factors can influence recovery, including: 1. the intensity of the pain at the beginning; 2. stress and anxiety; 3. fear of movement; 4. poor sleep; 5. fatigue; 6. lack of support from others; 7. difficulties at work or in daily life. All of these factors can affect how the body and brain respond to pain. Severe Pain at the Beginning: An Important Warning Sign When pain remains very intense for several days or weeks, it may be a sign that earlier intervention is needed. This does not mean that the situation is serious or that the pain will become permanent. However, it may indicate that additional support could help prevent the pain from becoming established. Chronic Pain Develops Gradually Chronic pain does not appear overnight. Over time, the nervous system can become more sensitive. The brain and nerves may then react more strongly to pain signals, even when the tissues are beginning to heal. This is why the first few weeks are important. The earlier action is taken, the better the chances of recovery. Certain Factors Can Slow Recovery When people are in pain, it is normal: · to be afraid of moving; · to avoid certain activities; · to feel discouraged; · to feel stressed or worried. These reactions are common. However, when they persist for a long time, they can make recovery more difficult. Healthcare professionals sometimes refer to these factors as “yellow flags.” Simple Tools to Better Support You Today, short questionnaires are available to help professionals better understand the risk of persistent pain. These tools help provide care that is adapted to each person’s needs. Some people may only need: · advice; · simple exercises; · and reassurance. Others may benefit from: · closer follow-up; · more comprehensive support; · or additional help managing pain. What Can Be Done to Support Recovery? Keep Moving Gradually Prolonged complete rest is rarely the best solution. Gentle movement and gradually returning to regular activities often help people recover more quickly. The important thing is to progress at your own pace. Understanding Pain Receiving clear and reassuring explanations can help: · reduce worries; · decrease fear of movement; · better manage symptoms. Understanding pain often helps people regain confidence in their bodies. Addressing Stress and Emotions Stress, anxiety, and certain negative thoughts can increase pain. In some cases, approaches such as: · relaxation; · stress management; · or psychological support can help improve recovery. Key Takeaways Persistent pain is not inevitable. Today, healthcare professionals have better tools to identify people who are at greater risk of developing chronic pain. The earlier care is adapted to the person’s needs, the better the chances of recovery. Early screening helps give people the best chance of preventing pain from becoming long-lasting. References: Artus, M., Campbell, P., Mallen, C. D., Dunn, K. M., van der Windt, D. A. (2017). Generic prognostic factors for musculoskeletal pain in primary care: A systematic review. BMJ Open, 7(1), e012901. https://doi.org/10.1136/bmjopen-2016-012901 Cohen, S. P., Vase, L., Hooten, W. M. (2021). Chronic pain: An update on burden, best practices, and new advances. The Lancet, 397(10289), 2082–2097. https://doi.org/10.1016/S0140-6736(21)00393-7 Daoust, R., Paquet, J., Cournoyer, A., Piette, É., Morris, J., Bhatt, M., Bhéreur, A., Bhatt, M. (2020). Relationship between acute pain trajectories after an emergency department visit and chronic pain: A Canadian prospective cohort study. BMJ Open, 10(12), e040390. https://doi.org/10.1136/bmjopen-2020-040390 Dowell, D., Ragan, K. R., Jones, C. M., Baldwin, G. T., Chou, R. (2022). CDC clinical practice guideline for prescribing opioids for pain — United States, 2022. MMWR Recommendations and Reports, 71(3), 1–95. https://doi.org/10.15585/mmwr.rr7103a1 Dunn, M., Rushton, A. B., Mistry, J., Soundy, A., Heneghan,
Une douleur au dos, au cou, à l’épaule ou au genou est très fréquente. Dans la majorité des cas, la douleur s’améliore avec le temps. Mais parfois, elle peut durer plusieurs mois et devenir chronique. La bonne nouvelle, c’est qu’il est souvent possible d’agir tôt pour réduire ce risque. Pourquoi certaines douleurs deviennent-elles chroniques ? La douleur ne dépend pas seulement d’une blessure ou d’un problème physique. Plusieurs facteurs peuvent influencer la récupération, notamment : 1. l’intensité de la douleur au départ; 2. le stress et l’anxiété; 3. la peur de bouger; 4. un mauvais sommeil; 5. la fatigue; 6. le manque de soutien autour de soi; 7. certaines difficultés au travail ou dans la vie quotidienne. Tous ces éléments peuvent avoir un impact sur la façon dont le corps et le cerveau réagissent à la douleur. Une douleur intense au départ : un signal important Lorsqu’une douleur reste très intense pendant plusieurs jours ou plusieurs semaines, cela peut être un signe qu’il faut intervenir plus rapidement. Cela ne veut pas dire que la situation est grave ou qu’elle deviendra permanente. Mais cela indique qu’un meilleur accompagnement pourrait être utile pour éviter que la douleur s’installe. La douleur chronique s’installe progressivement La douleur chronique n’apparaît pas du jour au lendemain. Avec le temps, le système nerveux peut devenir plus sensible. Le cerveau et les nerfs réagissent alors plus fortement aux signaux de douleur, même lorsque les tissus commencent à guérir. C’est pourquoi les premières semaines sont importantes. Plus on agit tôt, meilleures sont les chances de récupération. Certains facteurs peuvent ralentir la guérison Quand on a mal, il est normal : · d’avoir peur de bouger; · d’éviter certaines activités; · de se sentir découragé; · d’être stressé ou inquiet. Ces réactions sont fréquentes. Cependant, lorsqu’elles persistent longtemps, elles peuvent rendre la récupération plus difficile. Les professionnels de la santé appellent parfois ces facteurs des « drapeaux jaunes ». Des outils simples pour mieux vous aider Il existe aujourd’hui de courts questionnaires qui permettent aux professionnels de mieux comprendre le risque que la douleur persiste. Ces outils aident à offrir des soins adaptés aux besoins de chaque personne. Certaines personnes auront seulement besoin : · de conseils; · d’exercices simples; · et de réassurance. D’autres pourraient bénéficier : · d’un suivi plus rapproché; · d’un accompagnement plus global; · ou d’un soutien supplémentaire pour gérer la douleur. Que peut-on faire pour favoriser la récupération ? Continuer de bouger progressivement Le repos complet prolongé est rarement la meilleure solution. Bouger doucement et reprendre graduellement ses activités aide souvent à récupérer plus rapidement. L’important est d’avancer à son rythme. Comprendre la douleur Recevoir des explications claires et rassurantes peut aider à : · diminuer les inquiétudes; · réduire la peur du mouvement; · mieux gérer les symptômes. Comprendre la douleur permet souvent de reprendre confiance en son corps. Travailler aussi sur le stress et les émotions Le stress, l’anxiété et certaines pensées négatives peuvent amplifier la douleur. Dans certains cas, des approches comme : · la relaxation; · la gestion du stress; · ou un soutien psychologique peuvent aider à mieux récupérer. Ce qu’il faut retenir Une douleur persistante n’est pas une fatalité. Aujourd’hui, les professionnels de la santé disposent de meilleurs outils pour repérer les personnes plus à risque de développer une douleur chronique. Plus la prise en charge est adaptée tôt, meilleures sont les chances de récupération. Dépister tôt, c’est donner les meilleures chances d’éviter que la douleur s’installe durablement. Bibliographie Artus, M., Campbell, P., Mallen, C. D., Dunn, K. M., van der Windt, D. A. (2017). Generic prognostic factors for musculoskeletal pain in primary care: A systematic review. BMJ Open, 7(1), e012901. https://doi.org/10.1136/bmjopen-2016-012901 Cohen, S. P., Vase, L., Hooten, W. M. (2021). Chronic pain: An update on burden, best practices, and new advances. The Lancet, 397(10289), 2082–2097. https://doi.org/10.1016/S0140-6736(21)00393-7 Daoust, R., Paquet, J., Cournoyer, A., Piette, É., Morris, J., Bhatt, M., Bhéreur, A., Bhatt, M. (2020). Relationship between acute pain trajectories after an emergency department visit and chronic pain: A Canadian prospective cohort study. BMJ Open, 10(12), e040390. https://doi.org/10.1136/bmjopen-2020-040390 Dowell, D., Ragan, K. R., Jones, C. M., Baldwin, G. T., Chou, R. (2022). CDC clinical practice guideline for prescribing opioids for pain — United States, 2022. MMWR Recommendations and Reports, 71(3), 1–95. https://doi.org/10.15585/mmwr.rr7103a1 Dunn, M., Rushton, A. B., Mistry, J., Soundy, A., Heneghan,

La prévention de la chronicité des hernies discales

Le résumé de l'événement Défibrose 2026 au Kenya !

Labour pain is recognized as one of the most intense painful experiences a person may encounter in life (Zuarez-Easton et al., 2023). Although epidural analgesia is highly effective, it is not suitable for every situation or every patient preference. Expectations among women are changing. They now desire active involvement and minimal medical interventions during childbirth. According to the American College of Obstetricians and Gynecologists (ACOG), non-pharmacological methods are generally safe for the mother, fetus, and labour progression (Bryant Borders, 2019). TENS therefore fits naturally within this approach. TENS: A Simple Approach TENS uses low-intensity electrical currents to modulate pain transmission through inhibitory mechanisms of the central nervous system. In practical terms, it acts on pain perception without the use of pharmacological agents. In obstetrics, devices such as TENS-EVA have been developed specifically for labour pain. They are easy to use and, most importantly, allow the patient to control the intensity of stimulation according to her needs. Clear Evidence With Measurable Effects Recent studies provide a clearer understanding of the clinical impact of TENS. A meta-analysis published in 2025, including 51 randomized controlled trials and more than 10,000 participants, found an average reduction of approximately 2 points out of 10 on the visual analog pain scale among women using TENS compared with control groups (Hu et al., 2025). Moreover, approximately 52% of participants experienced substantial pain relief. This aligns with a previous systematic analysis that also found notable improvements in pain alleviation with TENS use (Thuvarakan et al., 2020). A Reassuring Safety Profile From a safety perspective, results are highly consistent across studies. Available data do not show an increase in adverse outcomes for either the mother or the newborn (Hu et al., 2025; Michalska et al., 2025). Additionally, research shows that using TENS does not lead to higher rates of Caesarean births, assisted vaginal deliveries, or other obstetrical interventions (Dowswell et al., 2009; Michalska et al., 2025). These findings are important, as they indicate that TENS can be integrated into clinical practice without altering labour progression or adding clinical risk. High Acceptability Among Patients Another significant aspect is the patient’s perspective. Approximately 63% of women who used TENS reported that they would choose to use it again in a future birth (Dowswell et al., 2009). This high level of acceptability is largely explained by the sense of control provided by the device. Being able to adjust the intensity independently according to one’s needs contributes to autonomy, a key component of the overall childbirth experience. The Role of TENS in Current Recommendations Guidelines from the American College of Obstetricians and Gynecologists acknowledge that TENS may contribute to labour pain management, although observed effects on pain scores vary across studies (Bryant Borders, 2019). For its part, the Cochrane review places greater emphasis on patient choice, stating that women should be able to use TENS at any stage of labour, either alone or alongside other methods (Dowswell et al., 2009). This position reflects the current shift toward more individualized care tailored to patient preferences. TENS is particularly relevant when integrated into a combined approach. It may be used alongside other interventions, whether pharmacological or non-pharmacological (Bryant Borders, 2019; Zuarez-Easton et al., 2023). This complementarity allows care to be adjusted to each patient’s needs without rigidity. What This Means in Practice In clinical settings, integrating TENS primarily broadens the range of available options. This is especially relevant when epidural analgesia is not possible or simply not desired. It is also a way to support a less interventionist approach by limiting medication use while preserving mobility and active participation during labour. Evidence also suggests that TENS is more effective when used early in labour. This highlights the importance of discussing it during the prenatal period so that patients can make informed decisions and feel comfortable using it when the time comes. Conclusion TENS-EVA represents a relevant non-pharmacological option supported by evidence. Its effect on pain is modest, but real and consistently observed across studies. This is combined with an excellent safety profile and strong patient acceptability, two particularly important considerations in obstetrical care. At a time when personalized care and respect for patient preferences are becoming increasingly central, TENS-EVA stands out as a valuable tool to integrate into practice. It broadens available options while supporting a patient-centred approach adapted to the reality of each birth. Références : Bernard, A., Oyler, D. R., Anglen, J. O., Burd, R. S., Khatri, V., Levy, M. J., Petersen, S. R., Sliker, C. W., Winchell, R. J. (2020). Best practices guidelines for acute pain management in trauma patients. American College of Surgeons. https://www.facs.org/quality-programs/trauma/tqp/center-programs/vrc/resources/ Bryant, A. S., Borders, A. E. (2019). Approaches to limit intervention during labor and birth. ACOG Committee Opinion No. 766. American College of Obstetricians and Gynecologists. Obstetrics Gynecology, 133(2), e164-e173. Dowswell, T., Bedwell, C., Lavender, T., Neilson, J. P. (2009). Transcutaneous electrical nerve stimulation (TENS) for pain relief in labour. Cochrane Database of Systematic Reviews, (2), CD007214. https://doi.org/10.1002/14651858.CD007214.pub2 Hu, Z. Y., Tang, J., Li, X. X., Zhang, Y., Wang, L., Chen, Y., Liu, Y., Wang, X. (2025). The efficacy and safety of transcutaneous electrical nerve stimulation for labor analgesia in the first stage of labor: A qualitative and quantitative analysis. Frontiers in Medicine, 13, 1730360. https://doi.org/10.3389/fmed.2026.1730360 Michalska, A., Blazuk-Fortak, A., Gladys-Jakubczyk, A., Wolder, D., Swiercz, G. (2025). The impact of transcutaneous electrical nerve stimulation (TENS) on the consecutive stages of labour and perinatal outcomes—A retrospective cohort study. Journal of Clinical Medicine, 14(10), 3445. https://doi.org/10.3390/jcm14103445 Thuvarakan, K., Zimmermann, H., Mikkelsen, M. K., Gazerani, P. (2020). Transcutaneous electrical nerve stimulation as a pain-relieving approach in labor pain: A systematic review and meta-analysis of randomized controlled trials. Neuromodulation: Journal of the International Neuromodulation Society, 23(6), 732-746. https://doi.org/10.1111/ner.13221 Zuarez-Easton, S., Erez, O., Zafran, N., Carmeli, S., Garmi, G., Salim, R. (2023). Pharmacologic and nonpharmacologic options for pain relief during labor: An expert review. American Journal of Obstetrics and Gynecology, 228(5S), S1246-S1259. https://doi.org/10.1016/j.ajog.2023.03.003