




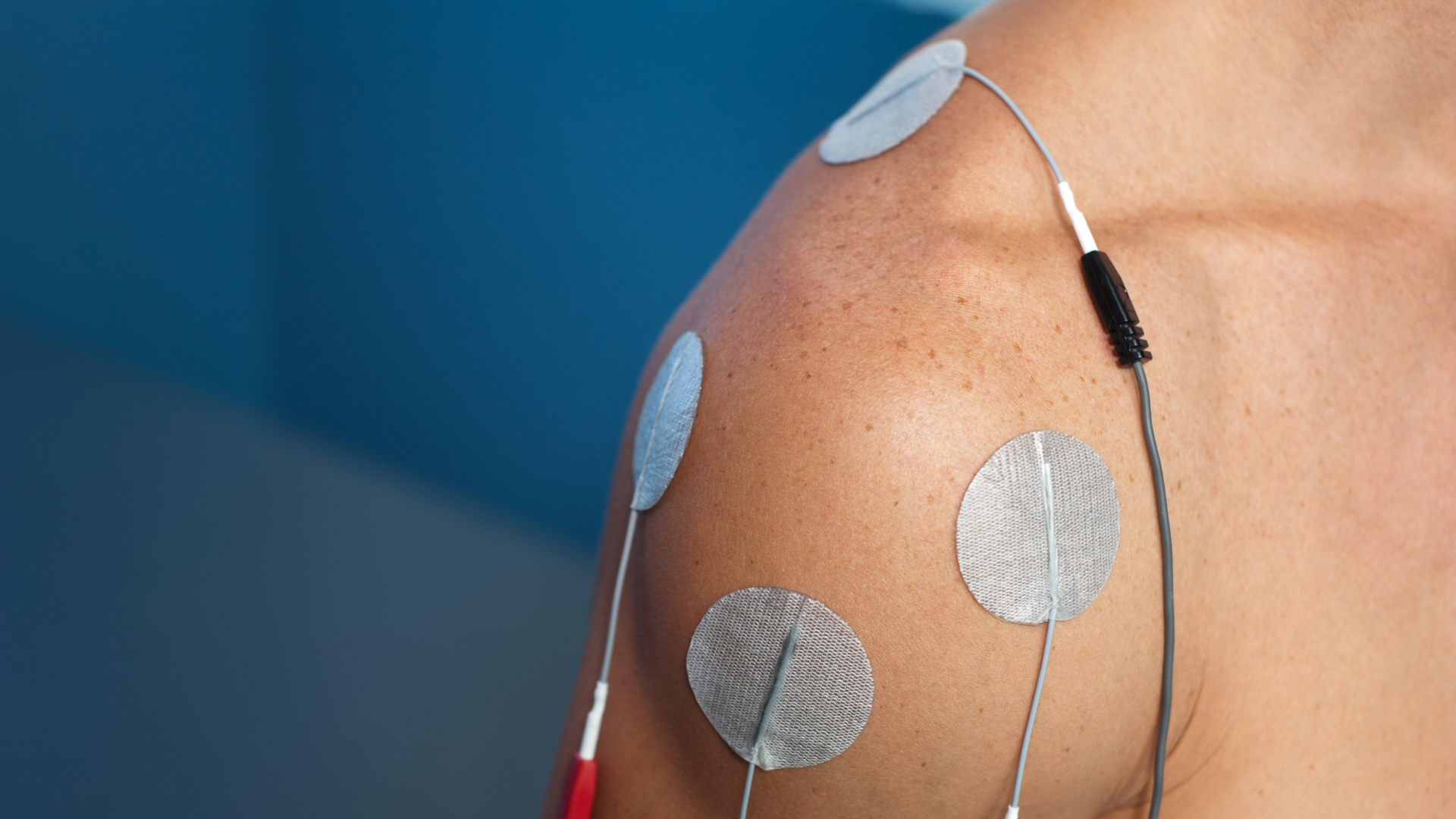
When we think of the postpartum period, pelvic floor recovery, muscle rehabilitation, and breastfeeding often come to mind. Yet, for many women, pain remains one of the greatest barriers to recovery. Pain may result from perineal trauma following vaginal birth, cesarean delivery, low back pain, neck and shoulder tension associated with breastfeeding, uterine cramping, or breastfeeding-related difficulties. These conditions can limit mobility, disrupt sleep, interfere with breastfeeding, and delay a return to daily activities. For healthcare professionals, this raises an important question: how can pain be managed effectively while ensuring treatment is safe, compatible with breastfeeding, and minimizes medication use whenever possible? EVA offers a promising solution. By combining transcutaneous electrical nerve stimulation (TENS) and neuromuscular electrical stimulation (NMES), it can address several conditions commonly encountered during the postpartum period. It may be used for both pain management and pelvic floor rehabilitation. However, the evidence supporting these applications varies. The following sections summarize what current research allows us to conclude. 1.Why TENS? TENS has been used for decades to treat musculoskeletal and postoperative pain. Its analgesic effects rely on two complementary mechanisms. At high frequencies, TENS stimulates large-diameter sensory (Aβ) fibers, reducing the transmission of nociceptive signals within the spinal cord through the gate control mechanism. At low frequencies, TENS activates descending inhibitory pathways and promotes the release of endogenous opioids. Together, these mechanisms contribute to longer-lasting analgesia (Smith et al., 2023). Recent evidence also suggests that TENS may influence inflammatory and immune responses. This mechanism may partly explain its benefits across a variety of pain conditions, including postpartum pain (Chen et al., 2025). 2.Perineal pain: the strongest evidence Perineal pain is currently the postpartum indication best supported by evidence for the use of TENS. A meta-analysis including 17 randomized controlled trials and nearly 2,000 participants found that TENS, when added to standard postpartum care, significantly reduced pain compared with standard care alone (Beleza et al., 2026). The certainty of the evidence was rated as moderate. This representing the strongest scientific support currently available for TENS in postpartum care. When TENS was compared with placebo, the findings also remained encouraging. However, the certainty of evidence was rated as very low because of methodological limitations. Clinical implications TENS can be incorporated into routine postpartum care alongside cryotherapy, positioning advice, therapeutic exercise, and analgesic medication when indicated. EVA therefore provides healthcare professionals with an additional non-pharmacological option for improving patient comfort without interfering with breastfeeding. 3.Post-cesarean pain: an adjunct to multimodal analgesia Pain after cesarean delivery can delay mobilization. It may also complicate newborn care and make breastfeeding more difficult. A Cochrane review of ten studies concluded that TENS reduces postoperative pain when used in addition to standard analgesia. Some studies also reported reduced use of rescue analgesics and improvements in physiological measures such as heart rate and respiratory rate (Zimpel et al., 2020). Clinical implications TENS is not intended to replace pharmacological analgesia. Rather, it can complement a multimodal pain management strategy aimed at improving pain control and promoting early mobilization. 4.Musculoskeletal pain: supporting functional recovery Low back, thoracic, and neck pain are common after childbirth. These symptoms are associated with pregnancy-related postural changes, infant care, breastfeeding, and the gradual return to daily activities. A review published in Frontiers in Neurology concluded that TENS effectively reduces several types of postpartum musculoskeletal pain while maintaining an excellent safety profile (Chen et al., 2025). Similarly, a network meta-analysis of pregnancy-related low back pain found significant improvements in physical function, with moderate-certainty evidence (Chen et al., 2021). Clinical implications EVA can complement therapeutic exercise, manual therapy, and postural education. Together, these interventions may promote a more comfortable recovery and facilitate a return to daily activities. 5.Pelvic floor rehabilitation: an additional advantage of EVA Pain is only one aspect of postpartum recovery. Many women also experience pelvic floor muscle weakness or difficulty activating these muscles effectively after childbirth. The NMES mode expands EVA's clinical applications. When neuromuscular electrical stimulation is indicated, it can support pelvic floor rehabilitation. For some patients, NMES may improve muscle awareness and facilitate muscle activation. It should be used alongside a supervised exercise program rather than as a stand-alone intervention. As with any rehabilitation strategy, NMES should be integrated into a comprehensive approach that includes clinical assessment, therapeutic exercise, and patient education. 6.Breast health: a promising area for future research Breastfeeding difficulties are another important source of postpartum pain. Plugged milk ducts, breast engorgement, and mastitis may interfere with breastfeeding and reduce quality of life. TENS is not currently recommended for these conditions. However, its potential is beginning to attract research interest. A case report by Smigelski and Gallagher described the use of TENS in a woman who experienced two episodes of plugged milk ducts. The authors reported rapid pain relief and complete resolution of the palpable breast mass after one or two treatment sessions. They hypothesized that electrical stimulation promoted contraction of the myoepithelial cells surrounding the mammary alveoli. This mechanism could facilitate milk ejection and help resolve ductal obstruction. How should these findings be interpreted? These findings are encouraging but should be interpreted cautiously. The report describes a single patient and did not include a control group. It also did not compare outcomes with the natural progression of the condition. Furthermore, outcomes relied primarily on patient-reported pain and clinical examination of the palpable mass. Consequently, no conclusions can be drawn regarding the effectiveness of TENS, and these findings cannot be generalized to breastfeeding women as a whole. The authors also emphasized that controlled clinical trials are needed before this approach can be recommended in clinical practice. 7.Key takeaways The postpartum period presents diverse and evolving clinical needs. Having a device that can address multiple aspects of recovery is therefore valuable for healthcare professionals. By combining TENS and NMES, EVA supports both pain management and pelvic floor rehabilitation. Current evidence particularly supports its use for: 1. Perineal pain following vaginal birth. 2. Post-cesarean pain. 3. Postpartum musculoskeletal pain. Other applications, particularly in breast health, remain investigational. Although preliminary findings are promising, high-quality clinical trials are needed before these indications can be incorporated into clinical practice guidelines. Overall, EVA is not a single solution for every postpartum challenge. Rather, it is a versatile device supported by evidence for several important indications. It can be integrated into a comprehensive, individualized, and woman-centred approach to postpartum care. Références: Beleza, A. C. S., Jorge, C. H., Liebano, R. E., et al. (2026). Electrophysical resources for the treatment of acute perineal pain after vaginal delivery: A systematic review with meta-analysis. The Journal of Pain. Bernard, A., Oyler, D. R., Anglen, J. O., et al. (2020). Best practices guidelines for acute pain management in trauma patients. American College of Surgeons. Chen, B., Chen, C., Zhao, X., & Xu, Y. (2025). An update comprehensive review on the effects of transcutaneous electrical nerve stimulation for postnatal physical and psychological disorders. Frontiers in Neurology. Chen, L., Ferreira, M. L., Beckenkamp, P. R., et al. (2021). Comparative efficacy and safety of conservative care for pregnancy-related low back pain: A systematic review and network meta-analysis. Physical Therapy. Deussen, A. R., Ashwood, P., Martis, R., Stewart, F., & Grzeskowiak, L. E. (2020). Relief of pain due to uterine cramping/involution after birth. Cochrane Database of Systematic Reviews. Gibson, W., Wand, B. M., Meads, C., Catley, M. J., & O'Connell, N. E. (2019). Transcutaneous electrical nerve stimulation (TENS) for chronic pain: An overview of Cochrane reviews. Cochrane Database of Systematic Reviews. Martimbianco, A. L. C., Porfírio, G. J., Pacheco, R. L., Torloni, M. R., & Riera, R. (2019). Transcutaneous electrical nerve stimulation (TENS) for chronic neck pain. Cochrane Database of Systematic Reviews. McCahill-Riley, M., Downey, K., & Clarke, V. (2026). Electrotherapy in lactation care. Journal of Human Lactation. Smith, T. J., Wang, E. J., & Loprinzi, C. L. (2023). Cutaneous electroanalgesia for relief of chronic and neuropathic pain. The New England Journal of Medicine. Smigelski, C., & Gallagher, L. (2024). The use of transcutaneous electrical nerve stimulation (TENS) to relieve pain and resolve blocked milk ducts in lactating women: A case report [Affiche scientifique]. Oregon Health & Science University. Zimpel, S. A., Torloni, M. R., Porfírio, G. J., Flumignan, R. L., & da Silva, E. M. (2020). Complementary and alternative therapies for post-caesarean pain. Cochrane Database of Systematic Reviews.
Neuromuscular electrical stimulation (NMES) is often associated with postoperative rehabilitation. However, growing evidence suggests that introducing NMES before surgery can play a meaningful role in improving patient outcomes (Punnoose et al., 2023; Walls et al., 2010; Patanè et al., 2025). This approach is based on a simple principle: the patient’s muscular status at the time of surgery influences postoperative recovery (Gillis et al., 2022; Hiyama et al., 2026). In other words, better preoperative muscle function is generally associated with better functional outcomes after surgery (Punnoose et al., 2023; Devasenapathy et al., 2019). This concept, often summarized as Better In, Better Out, is now supported by robust evidence across several orthopedic settings (Gillis et al., 2022; Jørgensen et al., 2024). Preoperative Muscle Strength: A Modifiable Prognostic Factor Among the many factors that influence recovery after orthopedic surgery, preoperative muscle strength stands out for two reasons. It is strongly associated with postoperative outcomes (Devasenapathy et al., 2019; Takamura et al., 2024; Hiyama et al., 2026), and it can be improved before surgery (Punnoose et al., 2023; Walls et al., 2010). Total Knee Arthroplasty In patients undergoing total knee arthroplasty, preoperative quadriceps strength is one of the strongest predictors of postoperative function (Devasenapathy et al., 2019; Hiyama et al., 2026). Patients with greater strength before surgery are more likely to achieve satisfactory mobility and functional recovery. Several studies have identified strength thresholds that predict walking ability six months after surgery (Takamura et al., 2024). More recently, Hiyama and colleagues (2026) reported that patients who regain age-adjusted normative quadriceps strength experience greater satisfaction and better functional outcomes one year after surgery. Anterior Cruciate Ligament Reconstruction A similar pattern is seen after anterior cruciate ligament reconstruction. Significant preoperative quadriceps weakness is associated with poorer knee function one year after surgery (Kim et al., 2022). Conversely, patients with greater preoperative strength tend to achieve better functional outcomes. These findings are consistent with the conclusions of a recent systematic review (Qiu et al., 2020). Shoulder Surgery Preoperative muscle strength also plays an important role in shoulder surgery. In patients undergoing anatomic or reverse shoulder arthroplasty, abduction and external rotation strength are among the strongest predictors of postoperative function (Hao et al., 2022a; Hao et al., 2022b). Grip strength, often considered a global indicator of muscle health and sarcopenia, has also been associated with outcomes following shoulder arthroplasty (Lee et al., 2023). More recent evidence suggests that it may also predict functional recovery after rotator cuff repair. NMES: An Opportunity Before Surgery If muscle strength affects postoperative outcomes, an obvious question arises: can this factor be optimized before surgery? NMES represents an attractive option, particularly for patients with pain, marked weakness, or functional limitations that restrict conventional exercise. In a pilot study involving patients awaiting total knee arthroplasty, a home-based NMES program increased quadriceps strength by approximately 28% before surgery (Walls et al., 2010). These gains translated into faster recovery of strength and function in the early postoperative period, while also limiting muscle atrophy. These findings align with the broader evidence supporting prehabilitation. A meta-analysis published in JAMA Network Open, which included 48 randomized controlled trials and more than 3,500 participants, found that preoperative interventions significantly improved muscle strength and physical function before surgery. Benefits persisted during the first weeks of postoperative recovery (Punnoose et al., 2023). The Role of NMES After Surgery NMES remains a valuable tool after surgery. During the early postoperative period, muscle recovery is limited by pain, joint effusion, immobilization, arthrogenic muscle inhibition, and reduced physical activity. In this context, NMES can effectively stimulate muscle activation despite these limitations. Following Knee Surgery After arthroplasty or ligament reconstruction, rapid quadriceps weakness represents a major clinical challenge. Early use of NMES may help attenuate strength loss and accelerate functional recovery, particularly when voluntary activation remains impaired. Following Shoulder Surgery Although evidence of preoperative NMES in shoulder surgery remains limited, postoperative findings are encouraging. Recent studies have shown that NMES may reduce deltoid atrophy after rotator cuff repair and accelerate recovery of abduction strength (Yoon et al., 2026). Other studies have reported earlier improvements in external rotation strength when NMES is applied to the infraspinatus during the initial phases of rehabilitation (Reinold et al., 2008). Sarcopenia: An Often Overlooked Factor Beyond muscle strength, preoperative muscle mass also appears to influence outcomes. A meta-analysis including more than 14,000 patients found that low preoperative muscle mass was associated with a significantly higher risk of major postoperative complications and short-term mortality (Weerink et al., 2020). In total knee arthroplasty, low muscle mass has also been identified as an independent risk factor for postoperative blood transfusion (Hwang et al., 2022). These findings highlight that preoperative preparation is not solely aimed at improving function. It may also help reduce surgical risk. Key Takeaways Current evidence points to a consistent conclusion: preoperative muscle status has a direct impact on recovery following orthopedic surgery. For rehabilitation professionals, this represents an opportunity to intervene before the operation takes place. NMES appears particularly valuable for optimizing a modifiable prognostic factor, especially when pain or functional limitations prevent patients from performing high-intensity strengthening exercises. From this perspective, the period leading up to surgery should no longer be viewed as passively waiting. Instead, it should be considered a therapeutic window during which clinicians can improve a patient’s muscle reserve, support postoperative recovery, and ultimately enhance functional outcomes. In orthopedic rehabilitation, recovery often begins long before the patient enters the operating room. References Bodkin, S. G., Norte, G. E., & Hart, J. M. (2019). Corticospinal excitability can discriminate quadriceps strength indicative of knee function after ACL-reconstruction. Scandinavian Journal of Medicine & Science in Sports, 29(5), 716–724. Devasenapathy, N., Maddison, R., Malhotra, R., Zodepy, S., & Sharma, S. (2019). Preoperative quadriceps muscle strength and functional ability predict performance-based outcomes 6 months after total knee arthroplasty: A systematic review. Physical Therapy, 99(1), 46–61. Gillis, C., Ljungqvist, O., & Carli, F. (2022). Prehabilitation, enhanced recovery after surgery, or both? A narrative review. British Journal of Anaesthesia, 128(3), 434–448. Hao, K. A., Wright, T. W., Schoch, B. S., Struk, A. M., King, J. J., & Farmer, K. W. (2022a). Association between preoperative shoulder strength and clinical outcomes after primary reverse total shoulder arthroplasty. Journal of the American Academy of Orthopaedic Surgeons, 30(15), e1035–e1044. Hao, K. A., Wright, T. W., Dean, E. W., Struk, A. M., & King, J. J. (2022b). Preoperative shoulder strength is associated with postoperative primary anatomic total shoulder arthroplasty outcomes and improvement. Journal of Shoulder and Elbow Surgery, 31(8), 1648–1656. Hauger, A. V., Reiman, M. P., Bjordal, J. M., Sheets, C., Ledbetter, L., & Goode, A. P. (2018). Neuromuscular electrical stimulation is effective in strengthening the quadriceps muscle after anterior cruciate ligament surgery. Knee Surgery, Sports Traumatology, Arthroscopy, 26(2), 399–410. Hiyama, Y., Sawa, R., Yokoyama, M., & Ishii, Y. (2026). Achieving normative quadriceps strength after total knee arthroplasty: Associations with satisfaction, function, and a predictive nomogram. The Bone & Joint Journal, 108-B(1), 45–52. Hwang, D., Han, H. S., Lee, M. C., & Ro, D. H. (2022). Low muscle mass is an independent risk factor for postoperative blood transfusion in total knee arthroplasty: A retrospective, propensity score-matched cohort study. BMC Geriatrics, 22(1), Article 137. Jenssen, K. K., Lundgreen, K., Madsen, J. E., Kvakestad, R., & Dimmen, S. (2018). Prognostic factors for functional outcome after rotator cuff repair: A prospective cohort study with 2-year follow-up. The American Journal of Sports Medicine, 46(14), 3504–3510. Jørgensen, S. L., Aagaard, P., Bohn, M. B., Mikkelsen, L. R., & Mechlenburg, I. (2024). The effect of blood flow restriction exercise prior to total knee arthroplasty on postoperative physical function, lower limb strength and patient-reported outcomes: A randomized controlled trial. Scandinavian Journal of Medicine & Science in Sports, 34(1), e14516. Kim, D. K., Park, G., Wang, J. H., Kuo, L. T., & Park, W. H. (2022). Preoperative quadriceps muscle strength deficit severity predicts knee function one year after anterior cruciate ligament reconstruction. Scientific Reports, 12(1), Article 11845. Lee, B. G., Lee, D., & Koh, J. H. (2023). Relationship between the preoperative grip strength and postoperative shoulder strength of patients treated via reverse shoulder arthroplasty. Journal of Shoulder and Elbow Surgery, 32(5), 1012–1019. Patanè, P., Carnevale Pellino, V., Febbi, M., Gatti, R., & Sirtori, V. (2025). Effects of a tele-prehabilitation program with indirect electrostimulation compared to home-based exercise in patients eligible for lower limb arthroplasty: A randomized controlled trial. Journal of Clinical Medicine, 14(3), Article 892. Punnoose, A., Claydon-Mueller, L. S., Weiss, O., Zhang, J., Maffulli, N., & Rushton, A. (2023). Takamura, D., Iwata, K., Yajima, Y., et al. (2024). Cut-off values of preoperative knee extensor strength and hip abductor strength for predicting good walking ability after total knee arthroplasty. Archives of Orthopaedic and Trauma Surgery, 144(1), 305–312. Walls, R. J., McHugh, G., O'Gorman, D. J., Moyna, N. M., & O'Byrne, J. M. (2010). Effects of preoperative neuromuscular electrical stimulation on quadriceps strength and functional recovery in total knee arthroplasty: A pilot study. BMC Musculoskeletal Disorders, 11, 119.

Pain in the back, neck, shoulder, or knee is very common. In most cases, pain improves over time. However, in some situations, it can last for several months and become chronic. The good news is that it is often possible to take action early to reduce this risk. Why Does Some Pain Become Chronic? Pain does not depend solely on an injury or a physical problem. Several factors can influence recovery, including: 1. the intensity of the pain at the beginning; 2. stress and anxiety; 3. fear of movement; 4. poor sleep; 5. fatigue; 6. lack of support from others; 7. difficulties at work or in daily life. All of these factors can affect how the body and brain respond to pain. Severe Pain at the Beginning: An Important Warning Sign When pain remains very intense for several days or weeks, it may be a sign that earlier intervention is needed. This does not mean that the situation is serious or that the pain will become permanent. However, it may indicate that additional support could help prevent the pain from becoming established. Chronic Pain Develops Gradually Chronic pain does not appear overnight. Over time, the nervous system can become more sensitive. The brain and nerves may then react more strongly to pain signals, even when the tissues are beginning to heal. This is why the first few weeks are important. The earlier action is taken, the better the chances of recovery. Certain Factors Can Slow Recovery When people are in pain, it is normal: · to be afraid of moving; · to avoid certain activities; · to feel discouraged; · to feel stressed or worried. These reactions are common. However, when they persist for a long time, they can make recovery more difficult. Healthcare professionals sometimes refer to these factors as “yellow flags.” Simple Tools to Better Support You Today, short questionnaires are available to help professionals better understand the risk of persistent pain. These tools help provide care that is adapted to each person’s needs. Some people may only need: · advice; · simple exercises; · and reassurance. Others may benefit from: · closer follow-up; · more comprehensive support; · or additional help managing pain. What Can Be Done to Support Recovery? Keep Moving Gradually Prolonged complete rest is rarely the best solution. Gentle movement and gradually returning to regular activities often help people recover more quickly. The important thing is to progress at your own pace. Understanding Pain Receiving clear and reassuring explanations can help: · reduce worries; · decrease fear of movement; · better manage symptoms. Understanding pain often helps people regain confidence in their bodies. Addressing Stress and Emotions Stress, anxiety, and certain negative thoughts can increase pain. In some cases, approaches such as: · relaxation; · stress management; · or psychological support can help improve recovery. Key Takeaways Persistent pain is not inevitable. Today, healthcare professionals have better tools to identify people who are at greater risk of developing chronic pain. The earlier care is adapted to the person’s needs, the better the chances of recovery. Early screening helps give people the best chance of preventing pain from becoming long-lasting. References: Artus, M., Campbell, P., Mallen, C. D., Dunn, K. M., van der Windt, D. A. (2017). Generic prognostic factors for musculoskeletal pain in primary care: A systematic review. BMJ Open, 7(1), e012901. https://doi.org/10.1136/bmjopen-2016-012901 Cohen, S. P., Vase, L., Hooten, W. M. (2021). Chronic pain: An update on burden, best practices, and new advances. The Lancet, 397(10289), 2082–2097. https://doi.org/10.1016/S0140-6736(21)00393-7 Daoust, R., Paquet, J., Cournoyer, A., Piette, É., Morris, J., Bhatt, M., Bhéreur, A., Bhatt, M. (2020). Relationship between acute pain trajectories after an emergency department visit and chronic pain: A Canadian prospective cohort study. BMJ Open, 10(12), e040390. https://doi.org/10.1136/bmjopen-2020-040390 Dowell, D., Ragan, K. R., Jones, C. M., Baldwin, G. T., Chou, R. (2022). CDC clinical practice guideline for prescribing opioids for pain — United States, 2022. MMWR Recommendations and Reports, 71(3), 1–95. https://doi.org/10.15585/mmwr.rr7103a1 Dunn, M., Rushton, A. B., Mistry, J., Soundy, A., Heneghan,

Labour pain is recognized as one of the most intense painful experiences a person may encounter in life (Zuarez-Easton et al., 2023). Although epidural analgesia is highly effective, it is not suitable for every situation or every patient preference. Expectations among women are changing. They now desire active involvement and minimal medical interventions during childbirth. According to the American College of Obstetricians and Gynecologists (ACOG), non-pharmacological methods are generally safe for the mother, fetus, and labour progression (Bryant Borders, 2019). TENS therefore fits naturally within this approach. TENS: A Simple Approach TENS uses low-intensity electrical currents to modulate pain transmission through inhibitory mechanisms of the central nervous system. In practical terms, it acts on pain perception without the use of pharmacological agents. In obstetrics, devices such as TENS-EVA have been developed specifically for labour pain. They are easy to use and, most importantly, allow the patient to control the intensity of stimulation according to her needs. Clear Evidence With Measurable Effects Recent studies provide a clearer understanding of the clinical impact of TENS. A meta-analysis published in 2025, including 51 randomized controlled trials and more than 10,000 participants, found an average reduction of approximately 2 points out of 10 on the visual analog pain scale among women using TENS compared with control groups (Hu et al., 2025). Moreover, approximately 52% of participants experienced substantial pain relief. This aligns with a previous systematic analysis that also found notable improvements in pain alleviation with TENS use (Thuvarakan et al., 2020). A Reassuring Safety Profile From a safety perspective, results are highly consistent across studies. Available data do not show an increase in adverse outcomes for either the mother or the newborn (Hu et al., 2025; Michalska et al., 2025). Additionally, research shows that using TENS does not lead to higher rates of Caesarean births, assisted vaginal deliveries, or other obstetrical interventions (Dowswell et al., 2009; Michalska et al., 2025). These findings are important, as they indicate that TENS can be integrated into clinical practice without altering labour progression or adding clinical risk. High Acceptability Among Patients Another significant aspect is the patient’s perspective. Approximately 63% of women who used TENS reported that they would choose to use it again in a future birth (Dowswell et al., 2009). This high level of acceptability is largely explained by the sense of control provided by the device. Being able to adjust the intensity independently according to one’s needs contributes to autonomy, a key component of the overall childbirth experience. The Role of TENS in Current Recommendations Guidelines from the American College of Obstetricians and Gynecologists acknowledge that TENS may contribute to labour pain management, although observed effects on pain scores vary across studies (Bryant Borders, 2019). For its part, the Cochrane review places greater emphasis on patient choice, stating that women should be able to use TENS at any stage of labour, either alone or alongside other methods (Dowswell et al., 2009). This position reflects the current shift toward more individualized care tailored to patient preferences. TENS is particularly relevant when integrated into a combined approach. It may be used alongside other interventions, whether pharmacological or non-pharmacological (Bryant Borders, 2019; Zuarez-Easton et al., 2023). This complementarity allows care to be adjusted to each patient’s needs without rigidity. What This Means in Practice In clinical settings, integrating TENS primarily broadens the range of available options. This is especially relevant when epidural analgesia is not possible or simply not desired. It is also a way to support a less interventionist approach by limiting medication use while preserving mobility and active participation during labour. Evidence also suggests that TENS is more effective when used early in labour. This highlights the importance of discussing it during the prenatal period so that patients can make informed decisions and feel comfortable using it when the time comes. Conclusion TENS-EVA represents a relevant non-pharmacological option supported by evidence. Its effect on pain is modest, but real and consistently observed across studies. This is combined with an excellent safety profile and strong patient acceptability, two particularly important considerations in obstetrical care. At a time when personalized care and respect for patient preferences are becoming increasingly central, TENS-EVA stands out as a valuable tool to integrate into practice. It broadens available options while supporting a patient-centred approach adapted to the reality of each birth. Références : Bernard, A., Oyler, D. R., Anglen, J. O., Burd, R. S., Khatri, V., Levy, M. J., Petersen, S. R., Sliker, C. W., Winchell, R. J. (2020). Best practices guidelines for acute pain management in trauma patients. American College of Surgeons. https://www.facs.org/quality-programs/trauma/tqp/center-programs/vrc/resources/ Bryant, A. S., Borders, A. E. (2019). Approaches to limit intervention during labor and birth. ACOG Committee Opinion No. 766. American College of Obstetricians and Gynecologists. Obstetrics Gynecology, 133(2), e164-e173. Dowswell, T., Bedwell, C., Lavender, T., Neilson, J. P. (2009). Transcutaneous electrical nerve stimulation (TENS) for pain relief in labour. Cochrane Database of Systematic Reviews, (2), CD007214. https://doi.org/10.1002/14651858.CD007214.pub2 Hu, Z. Y., Tang, J., Li, X. X., Zhang, Y., Wang, L., Chen, Y., Liu, Y., Wang, X. (2025). The efficacy and safety of transcutaneous electrical nerve stimulation for labor analgesia in the first stage of labor: A qualitative and quantitative analysis. Frontiers in Medicine, 13, 1730360. https://doi.org/10.3389/fmed.2026.1730360 Michalska, A., Blazuk-Fortak, A., Gladys-Jakubczyk, A., Wolder, D., Swiercz, G. (2025). The impact of transcutaneous electrical nerve stimulation (TENS) on the consecutive stages of labour and perinatal outcomes—A retrospective cohort study. Journal of Clinical Medicine, 14(10), 3445. https://doi.org/10.3390/jcm14103445 Thuvarakan, K., Zimmermann, H., Mikkelsen, M. K., Gazerani, P. (2020). Transcutaneous electrical nerve stimulation as a pain-relieving approach in labor pain: A systematic review and meta-analysis of randomized controlled trials. Neuromodulation: Journal of the International Neuromodulation Society, 23(6), 732-746. https://doi.org/10.1111/ner.13221 Zuarez-Easton, S., Erez, O., Zafran, N., Carmeli, S., Garmi, G., Salim, R. (2023). Pharmacologic and nonpharmacologic options for pain relief during labor: An expert review. American Journal of Obstetrics and Gynecology, 228(5S), S1246-S1259. https://doi.org/10.1016/j.ajog.2023.03.003

In clinical practice, the integration of new modalities must reflect real-world constraints, including limited time, patient adherence, and functional goals. Despite extensive research on neuromuscular electrical stimulation, its use remains limited or inconsistent. By gaining a deeper understanding of its applications, we can optimize its clinical effectiveness. 1 - What if strength loss could be limited from the early weeks? Following a major injury, such as anterior cruciate ligament reconstruction, recovery extends beyond tissue healing. The primary challenge lies in restoring function. Despite well-structured rehabilitation, many athletes present with persistent quadriceps weakness, muscle atrophy, and arthrogenic inhibition, which can delay progression. This raises an important clinical question: how can early rehabilitation be optimized to preserve muscle function and facilitate return to play? Neuromuscular electrical stimulation offers a practical and evidence-informed response to this challenge. 1.1 - Recruiting what exercise alone cannot activate The main value of neuromuscular electrical stimulation lies in its mechanism of action. Unlike voluntary contraction, it preferentially recruits type II muscle fibres, which are essential for force production and particularly vulnerable after injury. In the presence of arthrogenic inhibition, this capacity becomes especially relevant. This modality helps overcome limitations in voluntary activation and maintain sufficient muscular loading. It does not replace therapeutic exercise but rather enhances its effects. 1.2 - Measurable gains influencing return to sport The evidence supporting its use is high. For professional soccer players undergoing anterior cruciate ligament reconstruction, neuromuscular electrical stimulation has been proven to safely and effectively restore quadriceps muscle mass and strength. At the cellular level, early intervention has been shown to have positive outcomes. When initiated promptly after injury and continued for up to three weeks following surgery, it minimizes the atrophy of type II fibres and maintains the contractility of type I fibres. A randomized controlled trial also demonstrated that adding neuromuscular electrical stimulation to early sit-to-stand exercises, performed between 15 and 60 days postoperatively, improves quadriceps strength and reduces interlimb loading asymmetry at both 60 and 180 days. These outcomes are associated with a faster and safer return to sport. 2 - The motivational dimension: an important driver of rehabilitation Beyond its physiological effects, neuromuscular electrical stimulation offers a psychological benefit that is often overlooked: it helps sustain patient motivation throughout rehabilitation. 2.1 - Tangible results supporting engagement For athletes accustomed to high performance, the early postoperative period can be particularly challenging. Neuromuscular electrical stimulation enables meaningful muscle contractions, even when voluntary activation is limited by pain or arthrogenic inhibition. The ability to perceive muscle activation and observe measurable progress can strengthen patient confidence and support adherence to rehabilitation programs. Literature highlights the importance of psychological factors in return to sport. High motivation, strong psychological readiness, and low fear of reinjury are associated with a greater likelihood of returning to pre-injury levels. In this context, the effectiveness of neuromuscular electrical stimulation also depends on patient profile. Motivated individuals, for whom this modality is meaningful, are more likely to benefit. Athletes aiming for a rapid and safe return to play are therefore particularly appropriate candidates. Its integration should be guided by a shared decision-making approach that considers patient goals, preferences, and level of engagement. 2.2 - How to integrate neuromuscular electrical stimulation in clinical practice The effectiveness of neuromuscular electrical stimulation depends on how it is implemented. Four principles can guide its integration. Early implementation The first weeks represent a critical window. Early use helps limit muscle loss and supports quadriceps recovery. Combination with exercise Optimal results are achieved when stimulation is combined with functional exercises. Superimposing stimulation onto voluntary contractions, including both concentric and eccentric actions, can enhance strength gains. Parameter adjustment Stimulation parameters should be adapted to clinical objectives and the stage of rehabilitation. Moderate frequencies are commonly used for motor activation, with adjustments based on functional demands. Integration into a global return-to-play strategy Neuromuscular electrical stimulation is most effective when embedded within a structured and comprehensive approach. It should be combined with: • Gradual load progression • Objective performance measures • Assessment of psychological readiness • Mechanical stress quantification This alignment supports clinical decision-making and contributes to a safe return to sport. 3 - Key points for practice Neuromuscular electrical stimulation is a relevant tool for early intervention on muscle function. It can also support patient engagement and improve recovery trajectories. However, its effectiveness depends on alignment between the modality, patient goals, and motivation. Athletes engaged in a structured and goal-oriented return-to-play process are particularly appropriate candidates. When used alongside therapeutic exercise and integrated into a comprehensive strategy, it can enhance clinical outcomes. Its use should be guided by shared decision-making in order to support adherence and maximize long-term benefits. References: Ardern, C. L., Taylor, N. F., Feller, J. A., & Webster, K. E. (2013). A systematic review of the psychological factors associated with returning to sport following injury. British Journal of Sports Medicine, 47(17), 1120-1126. https://doi.org/10.1136/bjsports-2012-091203 Babault, N., Cometti, C., Maffiuletti, N. A., & Deley, G. (2011). Does electrical stimulation enhance post-exercise performance recovery? European Journal of Applied Physiology, 111(10), 2501-2507. https://doi.org/10.1007/s00421-011-2117-7 Ekizos, A., & Santuz, A. (2023). "Biofeedback-based return to sport": Individualization through objective assessments. Frontiers in Physiology, 14, 1185556. https://doi.org/10.3389/fphys.2023.1185556 Gabbett, T. J. (2020). How much? How fast? How soon? Three simple concepts for progressing training loads to minimize injury risk and enhance performance. The Journal of Orthopaedic and Sports Physical Therapy, 50(10), 570-573. https://doi.org/10.2519/jospt.2020.9256 Herring, S. A., Putukian, M., Kibler, W. B., et al. (2024). Team physician consensus statement: Return to sport/return to play and the team physician: A team physician consensus statement—2023 update. Medicine and Science in Sports and Exercise, 56(5), 767-775. https://doi.org/10.1249/MSS.0000000000003371 Hickey, J. T., Timmins, R. G., Maniar, N., Williams, M. D., & Opar, D. A. (2017). Criteria for progressing rehabilitation and determining return-to-play clearance following hamstring strain injury: A systematic review. Sports Medicine, 47(7), 1375-1387. https://doi.org/10.1007/s40279-016-0667-x Labanca, L., Rocchi, J. E., Laudani, L., et al. (2018). Neuromuscular electrical stimulation superimposed on movement early after ACL surgery. Medicine and Science in Sports and Exercise, 50(3), 407-416. https://doi.org/10.1249/MSS.0000000000001462 Malone, J. K., Blake, C., & Caulfield, B. M. (2014). Neuromuscular electrical stimulation during recovery from exercise: A systematic review. Journal of Strength and Conditioning Research, 28(9), 2478-2506. https://doi.org/10.1519/JSC.0000000000000426 Menezes, M. A., Menezes, D. A., Vasconcelos, L. L., & DeSantana, J. M. (2022). Is electrical stimulation effective in preventing or treating delayed-onset muscle soreness (DOMS) in athletes and untrained adults? A systematic review with meta-analysis. The Journal of Pain, 23(12), 2013-2035. https://doi.org/10.1016/j.jpain.2022.05.004 Taradaj, J., Halski, T., Kucharzewski, M., et al. (2013). The effect of neuromuscular electrical stimulation on quadriceps strength and knee function in professional soccer players: Return to sport after ACL reconstruction. BioMed Research International, 2013, 802534. https://doi.org/10.1155/2013/802534 Taylor, T., West, D. J., Howatson, G., et al. (2015). The impact of neuromuscular electrical stimulation on recovery after intensive, muscle damaging, maximal speed training in professional team sports players. Journal of Science and Medicine in Sport, 18(3), 328-332. https://doi.org/10.1016/j.jsams.2014.04.004 Toth, M. J., Tourville, T. W., Voigt, T. B., et al. (2020). Utility of neuromuscular electrical stimulation to preserve quadriceps muscle fiber size and contractility after anterior cruciate ligament injuries and reconstruction: A randomized, sham-controlled, blinded trial. The American Journal of Sports Medicine, 48(10), 2429-2437. https://doi.org/10.1177/0363546520933622

Pain can be concerning, especially when it persists. However, not all pain functions in the same way. Understanding the difference between acute and chronic pain can help you better understand what is happening in your body and choose appropriate strategies to improve your condition. Acute Pain: A Normal Warning Signal Acute pain is a normal bodily response to an injury, such as a sprain, fracture, or burn. It functions much like an alarm system, alerting you that a part of your body needs protection and time to heal. In general acute pain: · Is linked to a specific injury. · Gradually decreases as healing occurs. · Its course is often predictable In this context, the goal is to control pain while allowing the body adequate time to recover. Chronic Pain: When the System Becomes More Sensitive Pain is considered chronic when it persists beyond three months, even if the initial injury has healed or is healing. In such cases, there is not necessarily ongoing tissue damage. Rather, the nervous system may have become more sensitive. Nerves transmit signals more easily, and the brain may amplify these signals. This means that the pain is real, but it does not necessarily indicate an active injury. The body has become more vigilant or more sensitive. Understanding this distinction is important, as it can help reduce fear and better guide treatment. Why Early Pain Control Matters Although acute pain is normal, very intense or poorly controlled pain should not be ignored. Severe pain at the outset may increase the likelihood that it will persist. This does not mean that chronic pain will inevitably develop, but it highlights the importance of early and safe intervention. The objective is not only to improve immediate comfort, but also to support better long-term recovery. In rehabilitation, the aim is not solely to relieve pain, but also to provide you with tools to regain control. Medication Certain anti-inflammatory creams or gels may be helpful in the early stages. In some cases, oral medications such as acetaminophen or nonsteroidal anti-inflammatory drugs may also be recommended, depending on your situation. Your pharmacist can help you understand how to use these medications safely and effectively. Stronger medications, such as opioids, are generally not recommended as first-line treatments because of their associated risks. Your physician is best positioned to determine the most appropriate medication based on your specific condition. However, medication alone does not always eliminate pain completely. Complementary Modalities Nonpharmacological options are also commonly used in rehabilitation. For example, transcutaneous electrical nerve stimulation, known as TENS, is a device that delivers mild electrical impulses through the skin. Research indicates that it can reduce pain in the short term in both acute and chronic conditions. It may be used alone or in combination with other pharmacological or nonpharmacological treatments. Remaining actively engaged in your pain management process is essential. In rehabilitation, we can teach you: · Simple pain management strategies, such as the appropriate use of heat or cold and specific breathing techniques. · Exercises adapted to your stage of healing. · A gradual return to activities, with realistic goals. · Clear explanations of pain mechanisms to reduce fear and anxiety. These tools not only help reduce pain intensity, but also support confidence in your ability to move and function. Conclusion Acute and chronic pain do not function in the same way, and they are not managed in exactly the same manner. In all cases, your pain is taken seriously. The objective is to help you understand what is happening, reduce the intensity of your symptoms, and restore a sense of control. With an individualized, gradual, and appropriate approach, it is possible to improve your condition and support a meaningful and sustainable recovery. References: Cohen, S. P., Vase, L., & Hooten, W. M. (2021). Chronic pain : An update on burden, best practices, and new advances. Lancet, 397(10289), 2082‑2097. https://doi.org/10.1016/S0140-6736(21)00393-7 Hsu, J. R., Mir, H., Wally, M. K., Seymour, R. B., & Orthopaedic Trauma Association Musculoskeletal Pain Task Force. (2019). Clinical Practice Guidelines for Pain Management in Acute Musculoskeletal Injury. Journal of Orthopaedic Trauma, 33(5), e158‑e182. https://doi.org/10.1097/BOT.0000000000001430 Johnson, M. I. (2021). Resolving Long-Standing Uncertainty about the Clinical Efficacy of Transcutaneous Electrical Nerve Stimulation (TENS) to Relieve Pain : A Comprehensive Review of Factors Influencing Outcome. Medicina, 57(4), Article 4. https://doi.org/10.3390/medicina57040378 Johnson, M. I., Paley, C. A., Jones, G., Mulvey, M. R., & Wittkopf, P. G. (2022). Efficacy and safety of transcutaneous electrical nerve stimulation (TENS) for acute and chronic pain in adults : A systematic review and meta-analysis of 381 studies (the meta-TENS study). BMJ Open, 12(2), e051073. https://doi.org/10.1136/bmjopen-2021-051073 Nasir, A., Afridi, M., Afridi, O. K., Khan, M. A., Khan, A., Zhang, J., & Qian, B. (2025). The persistent pain enigma : Molecular drivers behind acute-to-chronic transition. Neuroscience and Biobehavioral Reviews, 173, 106162. https://doi.org/10.1016/j.neubiorev.2025.106162 Qaseem, A., McLean, R. M., O’Gurek, D., Batur, P., Lin, K., Kansagara, D. L., & for the Clinical Guidelines Committee of the American College of Physicians and the Commission on Health of the Public and Science of the American Academy of Family Physicians. (2020). Nonpharmacologic and Pharmacologic Management of Acute Pain From Non–Low Back, Musculoskeletal Injuries in Adults : A Clinical Guideline From the American College of Physicians and American Academy of Family Physicians. Annals of Internal Medicine, 173(9), 739‑748. https://doi.org/10.7326/M19-3602 Terminology | International Association for the Study of Pain. (s. d.). International Association for the Study of Pain (IASP). Consulté 16 février 2026, à l’adresse https://www.iasp-pain.org/resources/terminology/ Treede, R.-D., Rief, W., Barke, A., Aziz, Q., Bennett, M. I., Benoliel, R., Cohen, M., Evers, S., Finnerup, N. B., First, M. B., Giamberardino, M. A., Kaasa, S., Korwisi, B., Kosek, E., Lavand’homme, P., Nicholas, M., Perrot, S., Scholz, J., Schug, S., … Wang, S.-J. (2019). Chronic pain as a symptom or a disease : The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain, 160(1), 19‑27. https://doi.org/10.1097/j.pain.0000000000001384 VA/DoD, T. L. G. (s. d.). VA/DoD Clinical Practice Guideline for the Use of Opioids in the Management of Chronic Pain. Vase, L., Wager, T. D., & Eccleston, C. (2025). Opportunities for chronic pain self-management : Core psychological principles and neurobiological underpinnings. Lancet, 405(10491), 1781‑1790. https://doi.org/10.1016/S0140-6736(25)00404-0

A simple, safe, and evidence-based first-line approach Menstrual pain, commonly referred to as primary dysmenorrhea, is one of the most frequent causes of pelvic pain among adolescents and women of reproductive age. It typically presents as cramping pain that may persist for several hours to several days at the onset of menstruation. Although often regarded as a normal physiological phenomenon, primary dysmenorrhea is associated with substantial functional consequences, including reduced participation in daily activities, decreased work productivity, school absenteeism, and impaired quality of life (Arik et al., 2022; González-Mena et al., 2024). With respect to pharmacological management of primary dysmenorrhea, nonsteroidal anti-inflammatory drugs (NSAIDs) and hormonal therapies remain widely used. However, several authors have raised concerns regarding their optimal effectiveness, particularly in light of potential adverse effects or contraindications in certain patients (Elboim-Gabyzon & Kalichman, 2020; Han et al., 2024). These limitations have contributed to growing interest in nonpharmacological, affordable, and safe approaches, among which transcutaneous electrical nerve stimulation, commonly known as TENS, is gaining increasing recognition. TENS as a First-Line Option for Primary Dysmenorrhea TENS is a noninvasive modality that involves the application of low-intensity electrical currents through electrodes placed on the skin, typically over the abdominal or lumbar regions. This intervention is characterized by its ease of use, low cost, and potential for self-administration, allowing patients to maintain their daily activities during painful episodes (Elboim-Gabyzon & Kalichman, 2020). Current evidence supports the effectiveness of TENS in reducing pain associated with primary dysmenorrhea. A review of the literature has shown that TENS is more effective than placebo in alleviating menstrual pain (Arik et al., 2022). This meta-analysis synthesized findings from several randomized controlled trials. According to the most recent Cochrane systematic review, both high-frequency and low-frequency TENS may reduce pain compared with placebo or no treatment, although the level of certainty remains moderate due to methodological limitations in the included studies (Han et al., 2024). Beyond pain reduction, some studies have reported a decrease in analgesic use and an improved ability to maintain daily activities during menstruation. These outcomes are particularly relevant for the overall management of primary dysmenorrhea (Camilo et al., 2023; Han et al., 2024). Mechanisms of Action of TENS in Menstrual Pain Primary dysmenorrhea is primarily driven by excessive prostaglandin production, leading to uterine hypercontractility, local vasoconstriction, and transient myometrial ischemia. These processes contribute to painful cramping and heightened pain sensitivity during menstruation (Elboim-Gabyzon & Kalichman, 2020; González-Mena et al., 2024). TENS modulates menstrual pain through several complementary mechanisms. According to the gate control theory, stimulation of large-diameter afferent fibres inhibits the transmission of nociceptive signals at the level of the dorsal horn of the spinal cord, thereby reducing pain perception (Elboim-Gabyzon & Kalichman, 2020). In addition, TENS promotes the release of endogenous opioids, such as endorphins and enkephalins, contributing to central pain modulation (Han et al., 2024). It has also been hypothesized that TENS may exert indirect beneficial effects, including increased local circulation and reduced uterine ischemia. These mechanisms are consistent with the pathophysiology of primary dysmenorrhea, further supporting the relevance of TENS as an intervention that targets underlying contributors to menstrual pain (Elboim-Gabyzon & Kalichman, 2020). Safety of TENS The safety profile of TENS is well established in literature. Clinical studies and comprehensive reviews report a low incidence of adverse effects, which are generally mild and transient, such as minor skin redness at electrode sites (Han et al., 2024). No serious complications have been reported when standard contraindications are respected. The nonpharmacological nature of TENS represents a major clinical advantage, particularly for patients who experience poor tolerance to medications or who wish to limit their use of analgesics. Moreover, TENS can be used safely throughout the menstrual cycle, without concerns related to dependence or known drug interactions (Elboim-Gabyzon & Kalichman, 2020). Normalizing the Use of TENS Despite a growing body of supportive evidence, TENS remains underutilized in the management of primary dysmenorrhea. This situation is partly attributable to the persistent normalization of menstrual pain and the historical prioritization of pharmacological approaches. Normalizing the use of TENS requires acknowledging primary dysmenorrhea as a legitimate pain condition that warrants appropriate, accessible, and patient-centred pain management strategies. For health care professionals, integrating TENS as a first-line option offers an intervention that promotes patient autonomy, supports activity maintenance, and aligns with a multimodal approach to pain management. TENS may be used alone or in combination with other nonpharmacological interventions, such as therapeutic exercise, thermotherapy, or pain education, within a framework of individualized and evidence-based care (González-Mena et al., 2024; Mendes et al., 2024). Conclusion TENS represents a simple, safe, and effective option for pain management in primary dysmenorrhea. Current evidence suggests that initiating its use at the onset of symptoms may be particularly beneficial, especially for women seeking to maintain daily functioning while minimizing reliance on medications. By normalizing its use, health care professionals gain access to a practical tool to improve the management of menstrual pain and contribute to enhanced quality of life for those affected. Références Arik, M. I., Kiloatar, H., Aslan, B., & Icelli, M. (2022). The effect of TENS for pain relief in women with primary dysmenorrhea: A systematic review and meta-analysis. Explore, 18(2), 108–113. https://doi.org/10.1016/j.explore.2020.08.005 Camilo, F. M., Bossini, P. S., Driusso, P., Ávila, M. A., Parizotto, N. A., Sousa, U. R., & Ramos, R. R. (2023). The effects of electrode placement on analgesia using transcutaneous electrical nerve stimulation for primary dysmenorrhea: A single-blind randomized controlled clinical trial. Cureus, 15(5), e39326. https://doi.org/10.7759/cureus.39326 Elboim-Gabyzon, M., & Kalichman, L. (2020). Transcutaneous electrical nerve stimulation (TENS) for primary dysmenorrhea: An overview. International Journal of Women’s Health, 12, 1–10. https://doi.org/10.2147/IJWH.S220523 González-Mena, Á., Leirós-Rodríguez, R., & Hernández-Lucas, P. (2024). Treatment of women with primary dysmenorrhea with manual therapy and electrotherapy techniques: A systematic review and meta-analysis. Physical Therapy. https://doi.org/10.1093/ptj/pzae019 Han, S., Park, K. S., Lee, H., Kim, E., Zhu, X., Lee, J. M., & Suh, H. S. (2024). Transcutaneous electrical nerve stimulation (TENS) for pain control in women with primary dysmenorrhoea. Cochrane Database of Systematic Reviews, 2024(7), CD013331. https://doi.org/10.1002/14651858.CD013331.pub2 Mendes, C. F., Oliveira, L. S., Garcez, P. A., Azevedo-Santos, I. F., & DeSantana, J. M. (2024). Effect of different electric stimulation modalities on pain and functionality of patients with pelvic pain: A systematic review with meta-analysis. Pain Practice. https://doi.org/10.1111/papr.13417
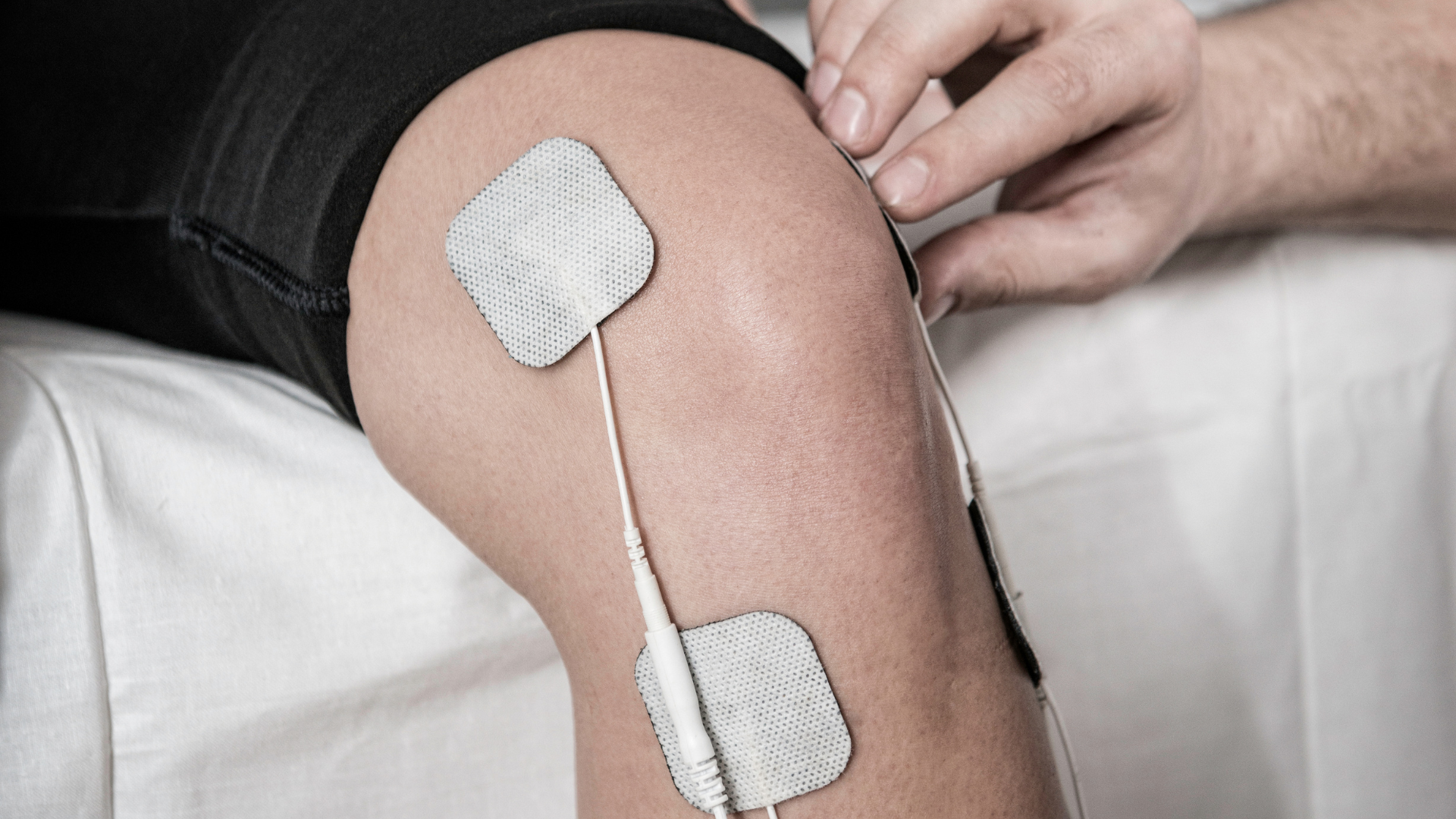
Neuromuscular electrical stimulation, commonly referred to as NMES, is widely used in rehabilitation to strengthen muscles with reduced voluntary activation. It can be used in conservative treatments and before, during, or after surgery. Its main advantage is its ability to activate motor units even in the presence of pain, swelling, or neuromuscular inhibition. Many muscles can benefit from NMES, but the quadriceps is the most studied because of its essential functional role and its sensitivity to arthrogenic inhibition, a protective reflex that decreases muscle activation when a joint is irritated or painful (Watson, 2020). The Scientific Foundations of NMES: A Distinct Mechanism of Motor Recruitment NMES stimulates motor nerves directly through an electrical current applied to the skin. It bypasses voluntary control and triggers muscle contraction by depolarizing axons. In normal physiology, small motor units are recruited first. With NMES, larger motor units are activated more quickly. These units are primarily type II fibres, which are faster and more powerful (Watson, 2020). This reversed recruitment pattern allows NMES to produce an effective contraction even when voluntary activation is limited by pain, arthrogenic inhibition, surgery, or immobilization. It helps prevent loss of muscle quality and supports functional recovery when voluntary effort is restricted. NMES also has motivational benefits. Patients who cannot voluntarily contract a muscle can observe a visible contraction produced by the device. This often reassures them and increases their engagement in rehabilitation. It can also reduce fear of movement and improve adherence to exercise programs. Optimal Timing of Use: From the Preoperative Period to Functional Recovery The Preoperative Period Muscle prehabilitation is associated with better postoperative outcomes (Anderson et al., 2021). NMES helps maintain function when pain or instability limits voluntary exercise (Watson, 2020). Although direct preoperative evidence is limited, early postoperative data suggest that regular stimulation preserves strength and reduces expected muscle loss (Watson, 2020). NMES therefore fits well into preoperative strengthening programs before ligament reconstruction or arthroplasty. The Early Postoperative Phase NMES is most effective when introduced soon after surgery. Conley et al. (2021) recommend starting within the first two postoperative weeks, when muscle inhibition is at its greatest. Early use improves quadriceps activation and accelerates strength recovery. A recent meta-analysis by Li et al. (2025) recommends beginning neuromuscular retraining within the first days after anterior cruciate ligament reconstruction. Early initiation is more effective than delayed application. This highlights the importance of early stimulation to optimize functional outcomes. The Intermediate Phase As pain decreases and mobility improves, NMES becomes a valuable adjunct to voluntary strengthening. It allows patients to reach contraction levels that they cannot achieve independently. When combined with exercise, NMES can increase strength and reduce pain, particularly at frequencies between 50 and 75 Hz (Novak et al., 2020). Its use depends on the targeted goals, such as strength, proprioception, or endurance. The Late Phase When patients can perform high-intensity exercises, NMES is used to support specific rehabilitation goals. It may help correct persistent imbalances, address residual deficits, or assist in monitoring mechanical load during a return to meaningful or sport-specific activities. Effects are generally more modest at this stage but remain useful. Peng et al. (2021) report moderate yet clinically relevant functional improvements after total knee arthroplasty. Conclusion: An Effective Modality When Applied at the Right Time NMES is most effective when integrated at appropriate stages of rehabilitation. In the preoperative period, it helps preserve muscle mass and quality. Immediately after surgery, it reduces neuromuscular inhibition and facilitates early reactivation of the targeted muscle. In later stages, it supports progressive strengthening, load monitoring, and optimization of muscle function. Regular use is essential for sustained benefits, much like a structured exercise program. Repetition and integration into self-management enhance its effectiveness. Finally, the extensive evidence available on the quadriceps provides a solid reference for clinical application and can be adapted to other muscle groups with appropriate judgment. References Watson, T. (2020) . Electrotherapy Evidence-Based Practice (13e éd.). Elsevier. Anderson, A. M., Comer, C., Smith, T. O., Drew, B. T., Pandit, H., Antcliff, D., Redmond, A. C., & McHugh, G. A. (2021). Consensus on pre-operative total knee replacement education and prehabilitation recommendations : A UK-based modified Delphi study. BMC Musculoskeletal Disorders, 22(1), 352. https://doi.org/10.1186/s12891-021-04160-5 Conley, C. E. W., Mattacola, C. G., Jochimsen, K. N., Dressler, E. V., Lattermann, C., & Howard, J. S. (2021). A Comparison of Neuromuscular Electrical Stimulation Parameters for Postoperative Quadriceps Strength in Patients After Knee Surgery : A Systematic Review. Sports Health: A Multidisciplinary Approach, 13(2), 116‑127. https://doi.org/10.1177/1941738120964817 Li, Z., Jin, L., Chen, Z., Shang, Z., Geng, Y., Tian, S., & Dong, J. (2025) . Effects of Neuromuscular Electrical Stimulation on Quadriceps Femoris Muscle Strength and Knee Joint Function in Patients After ACL Surgery : A Systematic Review and Meta-analysis of Randomized Controlled Trials. Orthopaedic Journal of Sports Medicine, 13(1), 23259671241275071. https://doi.org/10.1177/23259671241275071 Novak, S., Guerron, G., Zou, Z., Cheung, G., & Berteau, J.-P. (2020). New Guidelines for Electrical Stimulation Parameters in Adult Patients With Knee Osteoarthritis Based on a Systematic Review of the Current Literature. American Journal of Physical Medicine & Rehabilitation, 99(8), 682‑688. https://doi.org/10.1097/PHM.0000000000001409 Peng, L., Wang, K., Zeng, Y., Wu, Y., Si, H., & Shen, B. (2021) . Effect of Neuromuscular Electrical Stimulation After Total Knee Arthroplasty : A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Frontiers in Medicine, 8, 779019. https://doi.org/10.3389/fmed.2021.779019

Non-pharmacological strategies are taking on a growing place in pain management. In this context, transcutaneous electrical nerve stimulation, commonly known as TENS, is drawing renewed attention. Despite more than fifty years of research, its clinical effectiveness continues to provoke debate. Yet recent evidence shows that when this modality is properly understood and correctly applied, it can genuinely contribute to pain relief and to improved functional participation. For clinicians, understanding the mechanisms underlying TENS and the factors that shape its effectiveness allows for more accurate support of patient decision making and helps promote treatment adherence. 1- Back to basics, the gate control theory TENS is based on a concept introduced in the 1960s: the gate control theory proposed by Melzack and Wall. This model transformed the understanding of pain by demonstrating that nociceptive signals do not travel directly from the periphery to the brain. Rather, they pass through a modulatory center within the spinal cord, where they can be either amplified or attenuated. When a mild electrical current is applied to the skin, TENS activates nerve fibres associated with tactile and pressure sensations. These fibres conduct information more rapidly than nociceptive fibers, and their activation contributes to the “closing of the gate” to incoming pain signals, thereby reducing the amount of nociceptive input that reaches the brain. Most individuals perceive a comfortable tingling or vibrating sensation beneath the electrodes. This sensation reflects the activity of fibers that temporarily inhibit the transmission of pain impulses. In essence, TENS diminishes nociceptive signaling before the brain can interpret it. 2- Endorphin release The effects of TENS extend beyond the spinal gate. Electrical stimulation also elicits a chemical response, prompting the brain and spinal cord to release endogenous analgesic substances such as endorphins. These molecules act on the same receptors targeted by certain opioid medications, yet without producing their adverse effects. Research by Vance and colleagues indicates that the mechanisms engaged by TENS vary according to stimulation frequency. Low-frequency TENS promotes the release of endorphins, producing a more generalized and longer-lasting analgesic effect. High-frequency TENS, in contrast, acts on distinct neural circuits that inhibit pain more rapidly. Together, these mechanisms support the nervous system in regaining partial control over pain, which helps explain why some individuals experience relief that persists after the stimulation session. 3- Why stydy results vary Studies and systematic reviews on TENS frequently report heterogeneous findings. This variability largely reflects differences in how the modality is applied. Parameters such as intensity, frequency, duration, electrode placement and individual patient characteristics all influence treatment outcomes. These sources of variation help explain why some trials demonstrate marked benefits while others remain inconclusive. Intensity consistently emerges as the most critical parameter. For TENS to be effective, the stimulation must be sufficiently strong to generate a distinct yet comfortable sensation. If the intensity is too low, it will not activate the spinal gating mechanism nor promote the release of endogenous endorphins. Clinicians typically advise patients to increase the current until a stable, non-painful tingling is perceived, and to readjust it whenever the sensation diminishes. With repeated use, the nervous system may gradually adapt to stimulation, which can reduce its analgesic effect. Modifying the frequency, duration, or electrode placement often helps re-establish an adequate therapeutic response. Patient adherence is equally crucial. TENS is not a modality that can be prescribed and then left unattended. Individuals who understand when and how to use their device generally adjust the stimulation more effectively and obtain more meaningful outcomes. Conversely, insufficient instruction or follow-up often results in early discontinuation, which can be mistakenly interpreted as a lack of therapeutic efficacy. 4- What recent research shows Recent studies offer more compelling evidence of TENS effectiveness when the modality is applied appropriately. A 2022 meta-analysis conducted by Johnson and colleagues reported significant pain reduction across several conditions, including postoperative pain, knee osteoarthritis, chronic low back pain, diabetic neuropathy and fibromyalgia. In a separate study involving women with fibromyalgia, Vance and his team observed that participants who experienced improvement during the initial session were also those who showed the greatest benefit after several weeks of treatment. This finding suggests that early response may serve as a predictor of longer-term outcomes and underscores the importance of early follow-up and professional support. Together, these results indicate that TENS can be effective when intensity, frequency and clinical guidance are optimally aligned. 5- The clinician's role Although TENS can be used autonomously, its effectiveness relies heavily on the education and support provided by health professionals. The clinician must first assess whether TENS is suitable for the patient’s clinical presentation. Clinicians also play a central role in shared decision making. They outline the expected benefits, the limitations and the possibility that relief may be partial or temporary, thereby helping patients develop realistic expectations and reinforcing therapeutic trust. In addition, clinicians guide patients in electrode placement, in adjusting intensity and frequency and in identifying the most appropriate moments to use the device. Ultimately, TENS achieves its full therapeutic value when integrated into an active and collaborative clinician–patient relationship. 6- A tool for autonomy and participation When integrated into a multimodal treatment plan, TENS offers patients a concrete means of influencing their pain. This sense of control contributes meaningfully to adaptation and overall well-being. Although TENS does not replace core interventions such as exercise, rehabilitation or psychological approaches, it serves as a complementary modality that helps patients remain active. By supporting patients in understanding how TENS functions and how to adjust its parameters, clinicians foster autonomy and strengthen shared decision making. Ultimately, understanding TENS involves guiding patients toward informed choices that enhance their autonomy and their capacity to live well despite pain. References Travers, M. J., O’Connell, N. E., Tugwell, P., Eccleston, C., & Gibson, W. (2020). Transcutaneous electrical nerve stimulation (TENS) for chronic pain: The opportunity to begin again. The Cochrane Database of Systematic Reviews, 2020(4), ED000139. https://doi.org/10.1002/14651858.ED000139 Johnson, M. I. (2021). Resolving long-standing uncertainty about the clinical efficacy of transcutaneous electrical nerve stimulation (TENS) to relieve pain: A comprehensive review of factors influencing outcome. Medicina, 57(4), 378. https://doi.org/10.3390/medicina57040378 Johnson, M. I., Paley, C. A., Jones, G., Mulvey, M. R., Wittkopf, P. G., & Eardley, W. J. (2022). Efficacy and safety of transcutaneous electrical nerve stimulation (TENS) for acute and chronic pain in adults: A systematic review and meta-analysis of 381 studies (BMJ Open 2022;12:e051073). BMJ Open, 12(12), e051073. https://doi.org/10.1136/bmjopen-2021-051073 Vance, C. G. T., Dailey, D. L., Chimenti, R. L., Van Gorp, B. J., Crofford, L. J., & Sluka, K. A. (2022). Using TENS for pain control: Update on the state of the evidence. Medicina, 58(10), 1332. https://doi.org/10.3390/medicina58101332 Vance, C. G. T., Zimmerman, M. B., Dailey, D. L., Rakel, B. A., Geasland, K. M., Chimenti, R. L., Williams, J. M., Golchha, M., Crofford, L. J., & Sluka, K. A. (2021). Reduction in movement-evoked pain and fatigue during initial 30-minute transcutaneous electrical nerve stimulation treatment predicts TENS responders in women with fibromyalgia. Pain, 162(5), 1545–1555. https://doi.org/10.1097/j.pain.0000000000002144 Vance, C. G. T., Dailey, D. L., Rakel, B. A., & Sluka, K. A. (2014). Using TENS for pain control: The state of the evidence. Pain Management, 4(3), 197–209. https://doi.org/10.2217/pmt.14.13

Stay Active This Summer: Take Control with Self-Care Summer is the perfect time to explore, travel, get moving, and finally tackle all those projects that were on hold. Whether you're road-tripping, hiking, renovating, or simply soaking up the sun, this vibrant season invites us to push our limits and enjoy life to the fullest. But with increased activity often comes unexpected physical strain. Long hours on the road, repetitive movements, and intense efforts can quickly lead to discomfort or pain. When that happens, your body is sending a clear message: it’s time to act—before it disrupts your plans. The good news? You can take care of yourself right from home, without putting your summer on pause. Self-Care: Your Best Ally for an Active Summer Self-care is about listening to your body and taking proactive steps to maintain your well-being. It's a way to stay in control, especially when pain tries to slow you down. One of the most effective and user-friendly tools for self-care? The TENS unit. Why Choose TENS This Summer? TENS (Transcutaneous Electrical Nerve Stimulation) is a proven, drug-free method to relieve pain. It’s safe, easy to use, and fits perfectly into an active lifestyle. Here’s why it’s worth bringing along on your summer adventures: Fast and effective relief : Feel better in minutes, with results lasting between 2 to 8 hours. 100% natural, medication-free solution : No side effects—just relief. Discreet and portable : Wear it under your clothes while you go about your day. Stay active without compromise : Keep doing what you love, at your own pace. Supports professional care : Complements physiotherapy and rehabilitation treatments. Effective for various pain types : Including musculoskeletal, discogenic, and postural pain. Easy to use: no steep learning curve — you can start using it today, with guidance from healthcare professionals. Personalized and proactive pain management : Empower yourself to respond quickly and consistently. Listen to Your Body—and Keep Moving Pain doesn’t have to hold you back. With the right tools and a bit of guidance, you can enjoy all that summer has to offer—without sacrificing your comfort or well-being. By adding TENS to your daily routine, you’re taking a step toward freedom, movement, and greater autonomy over your health. Need advice or personalized support? Our experts are here to help you choose the right device and guide you in using it effectively. Get in touch with us today!